George Vasquez-Rios, John C Edwards, Saketh Tummala, Ashley Chapel, Ramez Sunna, David S Brink, Christopher Laohathai, Thanh-Mai Vo
{"title":"Immune reconstitution, glomerulonephritis, and successful treatment with rituximab.","authors":"George Vasquez-Rios, John C Edwards, Saketh Tummala, Ashley Chapel, Ramez Sunna, David S Brink, Christopher Laohathai, Thanh-Mai Vo","doi":"10.5414/CNCS110061","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Alemtuzumab can induce secondary autoimmunity affecting multiple organs. While kidney involvement is uncommon, it can be associated with devastating forms of glomerulonephritis (GN).</p><p><strong>Case presentation: </strong>A 32-year-old African American woman presented with hypertension, proteinuria, and progressive renal failure. Her medical history was remarkable for secondary progressive multiple sclerosis (SPMS). She had received her first induction dose of alemtuzumab 1 year prior to presentation. Upon evaluation, she had scanning speech, multidirectional nystagmus, and mild edema. Her serum creatinine was 2 mg/dL. Urine studies revealed proteinuria and microscopic hematuria. Her serologic tests were positive for c-antineutrophil cytoplasmic antibodies (> 1 : 640). In addition, she was found to have new-onset severe thyroid dysfunction with antibodies against thyroglobulin and thyroid peroxidase. Kidney biopsy was diagnostic for pauci-immune crescentic GN. The patient was treated with methylprednisolone and rituximab with subsequent renal, thyroid, and neurological recovery.</p><p><strong>Conclusion: </strong>This is an atypical case of GN following therapy with alemtuzumab. We hypothesize that immune reconstitution may be a potential mechanism. Alemtuzumab is a new treatment for SPMS that can be associated with GN. Practice guidelines should address the management of its renal complications.</p>","PeriodicalId":10398,"journal":{"name":"Clinical Nephrology. Case Studies","volume":"8 ","pages":"67-71"},"PeriodicalIF":0.0000,"publicationDate":"2020-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7469242/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Nephrology. Case Studies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5414/CNCS110061","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Alemtuzumab can induce secondary autoimmunity affecting multiple organs. While kidney involvement is uncommon, it can be associated with devastating forms of glomerulonephritis (GN).
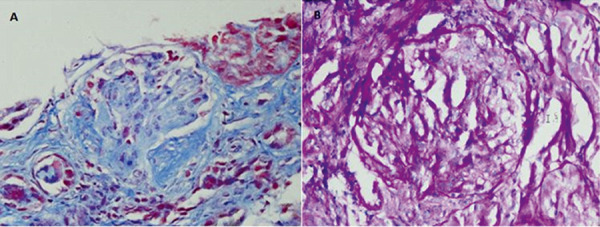
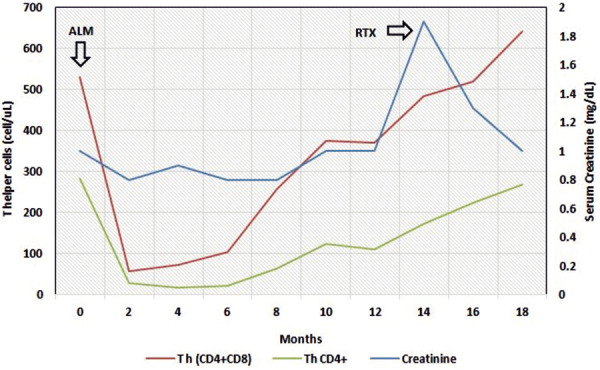
Case presentation: A 32-year-old African American woman presented with hypertension, proteinuria, and progressive renal failure. Her medical history was remarkable for secondary progressive multiple sclerosis (SPMS). She had received her first induction dose of alemtuzumab 1 year prior to presentation. Upon evaluation, she had scanning speech, multidirectional nystagmus, and mild edema. Her serum creatinine was 2 mg/dL. Urine studies revealed proteinuria and microscopic hematuria. Her serologic tests were positive for c-antineutrophil cytoplasmic antibodies (> 1 : 640). In addition, she was found to have new-onset severe thyroid dysfunction with antibodies against thyroglobulin and thyroid peroxidase. Kidney biopsy was diagnostic for pauci-immune crescentic GN. The patient was treated with methylprednisolone and rituximab with subsequent renal, thyroid, and neurological recovery.
Conclusion: This is an atypical case of GN following therapy with alemtuzumab. We hypothesize that immune reconstitution may be a potential mechanism. Alemtuzumab is a new treatment for SPMS that can be associated with GN. Practice guidelines should address the management of its renal complications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


