D V Shchukin, V N Lesovoy, G G Khareba, A I Harahatyi, A V Maltsev, M M Polyakov, R V Stetsyshyn, M P Kopytsya, P V Mozzhakov, O O Makovozov
{"title":"Removal of the Tumor Thrombus from the Right Atrium without Extracorporeal Circulation: Emphasis on the Displacement of the Tumor Apex.","authors":"D V Shchukin, V N Lesovoy, G G Khareba, A I Harahatyi, A V Maltsev, M M Polyakov, R V Stetsyshyn, M P Kopytsya, P V Mozzhakov, O O Makovozov","doi":"10.1155/2020/6063018","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To assess the outcomes of cavoatrial tumor thrombus removal using the liver transplantation technique for thrombectomy, a retrospective study was conducted.</p><p><strong>Materials and methods: </strong>Five patients with atrial tumor thrombi who underwent piggy-back mobilization of the liver, surgical access to the right atrium from the abdominal cavity, and external manual repositioning of the thrombus apex below the diaphragm (milking maneuver) were included into the study. Extracorporeal circulation was used in none of the cases. The average length of the atrial component of the tumor was 20.0 ± 11.7 mm (10 to 35 mm), and the width was 14.8 ± 8.5 mm (10 to 30 mm). In this work, the features of patients and surgical interventions as well as perioperative complications and mortality were analyzed.</p><p><strong>Results: </strong>External manual repositioning of the tumor thrombus apex below the diaphragm was successfully performed in all patients. Tumor thrombi with the length of the atrial part up to 1.5 cm were removed through the extrapericardial approach. For evacuation of the thrombi with the large atrial part (3.0 cm or more), a transpericardial surgical approach was required. Specific complications associated with the access to the right atrium from the abdominal cavity (paresis of the right phrenic nerve, pneumothorax, and mediastinitis) were not detected in any case. The average clamping time of the supradiaphragmatic inferior vena cava (IVC) was 6.3 ± 4.6 min. The volume of intraoperative blood loss varied from 2500 to 5600 ml (an average of 3675 ± 1398.5 ml).</p><p><strong>Conclusion: </strong>Our work represents the initial experience in the liver transplantation technique for thrombectomy in distinct and well-selected patients with atrial tumor thrombi. The effectiveness of this approach needs further study. The video presentation of our research took place in March 2019 at the 34th Annual EAU Congress in Barcelona.</p>","PeriodicalId":7490,"journal":{"name":"Advances in Urology","volume":" ","pages":"6063018"},"PeriodicalIF":2.3000,"publicationDate":"2020-06-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2020/6063018","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/6063018","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 3
Abstract
Objectives: To assess the outcomes of cavoatrial tumor thrombus removal using the liver transplantation technique for thrombectomy, a retrospective study was conducted.
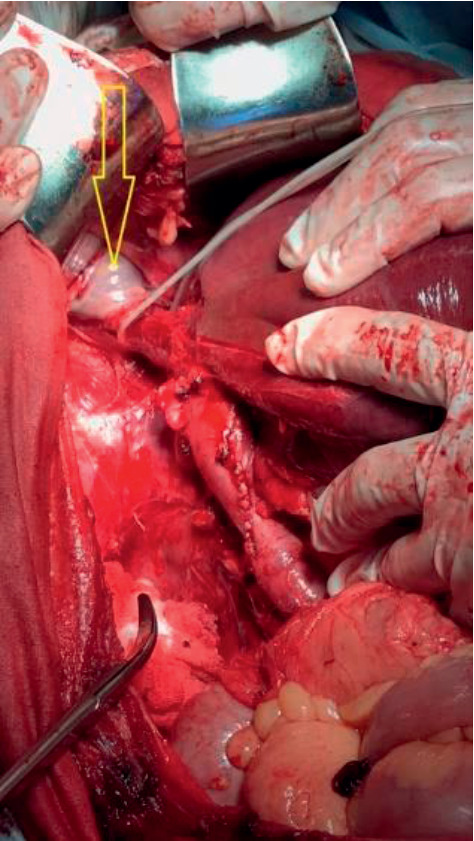
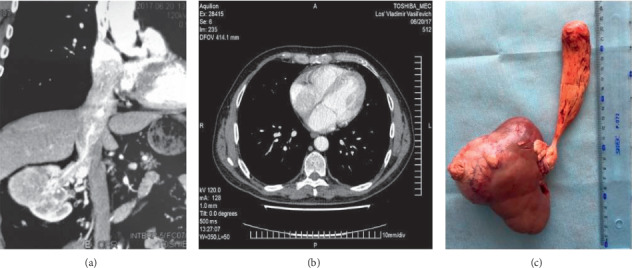
Materials and methods: Five patients with atrial tumor thrombi who underwent piggy-back mobilization of the liver, surgical access to the right atrium from the abdominal cavity, and external manual repositioning of the thrombus apex below the diaphragm (milking maneuver) were included into the study. Extracorporeal circulation was used in none of the cases. The average length of the atrial component of the tumor was 20.0 ± 11.7 mm (10 to 35 mm), and the width was 14.8 ± 8.5 mm (10 to 30 mm). In this work, the features of patients and surgical interventions as well as perioperative complications and mortality were analyzed.
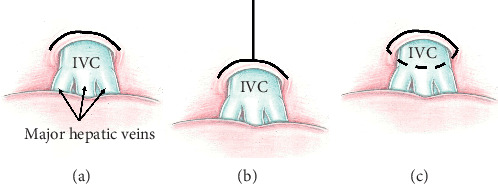
Results: External manual repositioning of the tumor thrombus apex below the diaphragm was successfully performed in all patients. Tumor thrombi with the length of the atrial part up to 1.5 cm were removed through the extrapericardial approach. For evacuation of the thrombi with the large atrial part (3.0 cm or more), a transpericardial surgical approach was required. Specific complications associated with the access to the right atrium from the abdominal cavity (paresis of the right phrenic nerve, pneumothorax, and mediastinitis) were not detected in any case. The average clamping time of the supradiaphragmatic inferior vena cava (IVC) was 6.3 ± 4.6 min. The volume of intraoperative blood loss varied from 2500 to 5600 ml (an average of 3675 ± 1398.5 ml).
Conclusion: Our work represents the initial experience in the liver transplantation technique for thrombectomy in distinct and well-selected patients with atrial tumor thrombi. The effectiveness of this approach needs further study. The video presentation of our research took place in March 2019 at the 34th Annual EAU Congress in Barcelona.
期刊介绍:
Advances in Urology is a peer-reviewed, open access journal that publishes state-of-the-art reviews and original research papers of wide interest in all fields of urology. The journal strives to provide publication of important manuscripts to the widest possible audience worldwide, without the constraints of expensive, hard-to-access, traditional bound journals. Advances in Urology is designed to improve publication access of both well-established urologic scientists and less well-established writers, by allowing interested scientists worldwide to participate fully.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


