Steven Deitelzweig, Christine L Baker, Amol D Dhamane, Jack Mardekian, Oluwaseyi Dina, Lisa Rosenblatt, Cristina Russ, Tayla Poretta, Melissa Lingohr-Smith, Jay Lin
{"title":"Comparison of readmissions among hospitalized nonvalvular atrial fibrillation patients treated with oral anticoagulants in the United States.","authors":"Steven Deitelzweig, Christine L Baker, Amol D Dhamane, Jack Mardekian, Oluwaseyi Dina, Lisa Rosenblatt, Cristina Russ, Tayla Poretta, Melissa Lingohr-Smith, Jay Lin","doi":"10.1080/21556660.2020.1750418","DOIUrl":null,"url":null,"abstract":"<p><p><b>Objectives:</b> To compare the risks of 1-month all-cause, major bleeding (MB)-related and stroke-related readmissions and the associated hospital resource use and costs among patients previously hospitalized for nonvalvular atrial fibrillation (NVAF) and treated with warfarin, rivaroxaban, and dabigatran vs apixaban. <b>Methods:</b> Adult patients hospitalized with NVAF (any discharge diagnosis position) who received apixaban, warfarin, rivaroxaban, or dabigatran during hospitalization were identified from the Premier database (1 January 2013-30 June 2017) and grouped into respective cohorts. Propensity score matching was used to generate cohorts with similar characteristics. In regression analyses the risk of readmissions that occurred within 1 month of discharge were evaluated and the associated length of stay (LOS) and costs compared. <b>Results:</b> NVAF patients treated with warfarin vs apixaban had significantly greater risk of all-cause (odds ratio [OR] = 1.05; confidence interval [CI] = 1.02-1.08; <i>p</i> < .001), MB-related (OR: 1.28; CI: 1.16-1.42; <i>p</i> < .001), and stroke-related (OR: 1.33; CI: 1.11-1.58; <i>p</i> = .002) readmissions; for all readmission categories, average LOS was significantly longer and costs significantly higher for warfarin treated patients. NVAF patients treated with rivaroxaban versus apixaban had significantly greater risk of all-cause (OR: 1.06; CI: 1.02-1.09; <i>p</i> = .001) and MB-related (OR = 1.62; CI = 1.44-1.83; <i>p</i> < .001) readmissions, but not stroke-related readmission; for MB-related readmissions average LOS and costs were higher for rivaroxaban treated patients. Significant differences in risks of all-cause, MB-related, and stroke-related readmissions were not observed between the apixaban and dabigatran cohorts. <b>Conclusion:</b> In this retrospective real-world analysis of NVAF patients, apixaban treatment was associated with better clinical outcomes than warfarin or rivaroxaban and lower hospital resource burden.</p>","PeriodicalId":15631,"journal":{"name":"Journal of Drug Assessment","volume":"9 1","pages":"87-96"},"PeriodicalIF":2.4000,"publicationDate":"2020-04-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1080/21556660.2020.1750418","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Drug Assessment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/21556660.2020.1750418","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
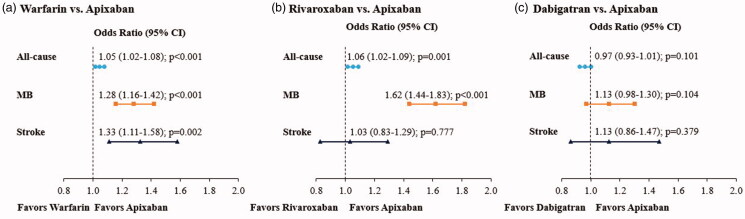
Objectives: To compare the risks of 1-month all-cause, major bleeding (MB)-related and stroke-related readmissions and the associated hospital resource use and costs among patients previously hospitalized for nonvalvular atrial fibrillation (NVAF) and treated with warfarin, rivaroxaban, and dabigatran vs apixaban. Methods: Adult patients hospitalized with NVAF (any discharge diagnosis position) who received apixaban, warfarin, rivaroxaban, or dabigatran during hospitalization were identified from the Premier database (1 January 2013-30 June 2017) and grouped into respective cohorts. Propensity score matching was used to generate cohorts with similar characteristics. In regression analyses the risk of readmissions that occurred within 1 month of discharge were evaluated and the associated length of stay (LOS) and costs compared. Results: NVAF patients treated with warfarin vs apixaban had significantly greater risk of all-cause (odds ratio [OR] = 1.05; confidence interval [CI] = 1.02-1.08; p < .001), MB-related (OR: 1.28; CI: 1.16-1.42; p < .001), and stroke-related (OR: 1.33; CI: 1.11-1.58; p = .002) readmissions; for all readmission categories, average LOS was significantly longer and costs significantly higher for warfarin treated patients. NVAF patients treated with rivaroxaban versus apixaban had significantly greater risk of all-cause (OR: 1.06; CI: 1.02-1.09; p = .001) and MB-related (OR = 1.62; CI = 1.44-1.83; p < .001) readmissions, but not stroke-related readmission; for MB-related readmissions average LOS and costs were higher for rivaroxaban treated patients. Significant differences in risks of all-cause, MB-related, and stroke-related readmissions were not observed between the apixaban and dabigatran cohorts. Conclusion: In this retrospective real-world analysis of NVAF patients, apixaban treatment was associated with better clinical outcomes than warfarin or rivaroxaban and lower hospital resource burden.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


