Victor C K Lo, Haitong Su, Yuet Ming Lam, Kathleen Willis, Virginia Pullar, Matthew Kowgier, Ryan P Hubner, Jennifer L Y Tsang
{"title":"Management of Patients With Sepsis in Canadian Community Emergency Departments: A Retrospective Multicenter Observational Study.","authors":"Victor C K Lo, Haitong Su, Yuet Ming Lam, Kathleen Willis, Virginia Pullar, Matthew Kowgier, Ryan P Hubner, Jennifer L Y Tsang","doi":"10.1177/2333392820920082","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Sepsis is a life-threatening syndrome and a leading cause of morbidity and mortality representing significant financial burden on the health-care system. Early identification and intervention is crucial to maximizing positive outcomes. We studied a quality improvement initiative with the aim of reviewing the initial management of patients with sepsis in Canadian community emergency departments, to identify areas for improving the delivery of sepsis care. We present a retrospective, multicenter, observational study during 2011 to 2015 in the community setting.</p><p><strong>Methods: </strong>We collected data on baseline characteristics, clinical management metrics (triage-to-physician-assessment time, triage-to-lactate-drawn time, triage-to-antibiotic time, and volume of fluids administered within the first 6 hours of triage), and outcomes (intensive care unit [ICU] admission, in-hospital mortality) from a regional database.</p><p><strong>Results: </strong>A total of 2056 patients were analyzed. The median triage-to-physician-assessment time was 50 minutes (interquartile range [IQR]: 25-104), triage-to-lactate-drawn time was 50 minutes (IQR: 63-94), and triage-to-antibiotics time was 129 minutes (IQR: 70-221). The median total amount of fluid administered within 6 hours of triage was 2.0 L (IQR: 1.5-3.0). The ICU admission rate was 36% and in-hospital mortality was 25%. We also observed a higher ICU admission rate (51% vs 24%) and in-hospital mortality (44% vs 14%) in those with higher lactate concentration (≥4 vs ≤2 mmol/L), independent of other sepsis-related parameters.</p><p><strong>Conclusion: </strong>Time-to-physician-assessment, time-to-lactate-drawn, time-to-antibiotics, and fluid resuscitation in community emergency departments could be improved. Future quality improvement interventions are required to optimize management of patients with sepsis. Elevated lactate concentration was also independently associated with ICU admission rate and in-hospital mortality rate.</p>","PeriodicalId":12951,"journal":{"name":"Health Services Research and Managerial Epidemiology","volume":"7 ","pages":"2333392820920082"},"PeriodicalIF":1.5000,"publicationDate":"2020-04-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/2333392820920082","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Services Research and Managerial Epidemiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2333392820920082","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Sepsis is a life-threatening syndrome and a leading cause of morbidity and mortality representing significant financial burden on the health-care system. Early identification and intervention is crucial to maximizing positive outcomes. We studied a quality improvement initiative with the aim of reviewing the initial management of patients with sepsis in Canadian community emergency departments, to identify areas for improving the delivery of sepsis care. We present a retrospective, multicenter, observational study during 2011 to 2015 in the community setting.
Methods: We collected data on baseline characteristics, clinical management metrics (triage-to-physician-assessment time, triage-to-lactate-drawn time, triage-to-antibiotic time, and volume of fluids administered within the first 6 hours of triage), and outcomes (intensive care unit [ICU] admission, in-hospital mortality) from a regional database.
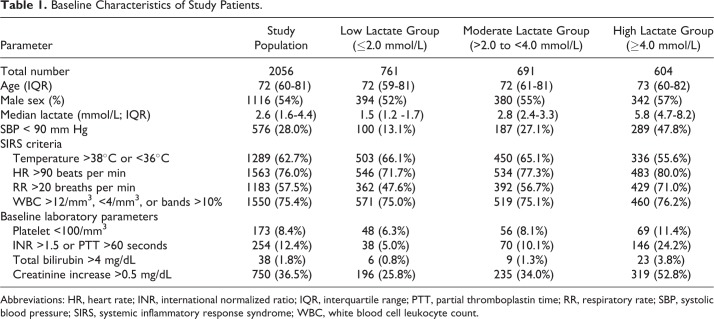
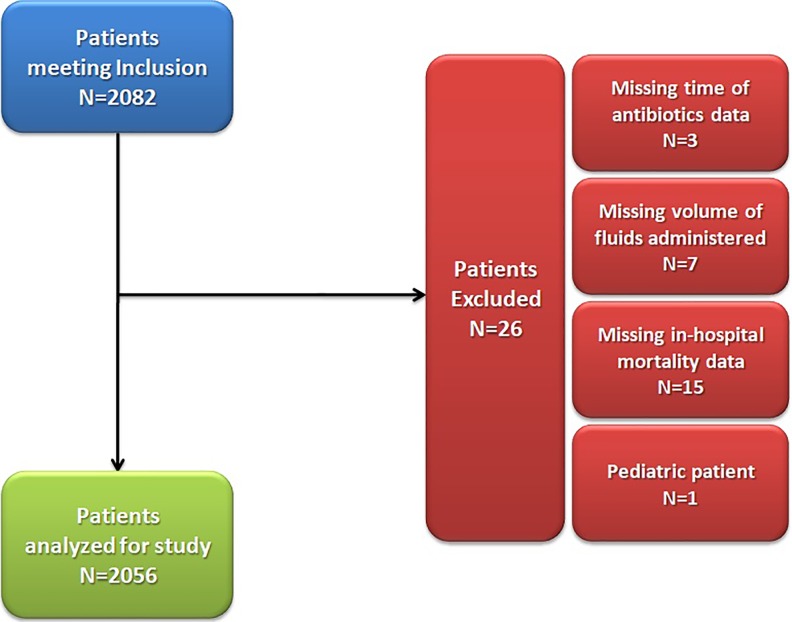
Results: A total of 2056 patients were analyzed. The median triage-to-physician-assessment time was 50 minutes (interquartile range [IQR]: 25-104), triage-to-lactate-drawn time was 50 minutes (IQR: 63-94), and triage-to-antibiotics time was 129 minutes (IQR: 70-221). The median total amount of fluid administered within 6 hours of triage was 2.0 L (IQR: 1.5-3.0). The ICU admission rate was 36% and in-hospital mortality was 25%. We also observed a higher ICU admission rate (51% vs 24%) and in-hospital mortality (44% vs 14%) in those with higher lactate concentration (≥4 vs ≤2 mmol/L), independent of other sepsis-related parameters.
Conclusion: Time-to-physician-assessment, time-to-lactate-drawn, time-to-antibiotics, and fluid resuscitation in community emergency departments could be improved. Future quality improvement interventions are required to optimize management of patients with sepsis. Elevated lactate concentration was also independently associated with ICU admission rate and in-hospital mortality rate.
背景:败血症是一种危及生命的综合征,是发病率和死亡率的主要原因,对卫生保健系统构成了重大的经济负担。早期识别和干预对于最大化积极结果至关重要。我们研究了一项质量改进倡议,目的是回顾加拿大社区急诊科败血症患者的初始管理,以确定改进败血症护理的领域。我们在2011年至2015年在社区环境中进行了一项回顾性、多中心、观察性研究。方法:我们从区域数据库收集基线特征、临床管理指标(分诊到医生评估时间、分诊到抽乳酸时间、分诊到抗生素时间、分诊前6小时内给液量)和结果(重症监护病房[ICU]入院、住院死亡率)的数据。结果:共分析2056例患者。从分诊到医生评估的中位数时间为50分钟(四分位数间距[IQR]: 25-104),从分诊到抽乳酸时间为50分钟(IQR: 63-94),从分诊到抗生素时间为129分钟(IQR: 70-221)。分诊6小时内给予的液体总量中位数为2.0 L (IQR: 1.5-3.0)。ICU住院率为36%,住院死亡率为25%。我们还观察到,与其他败血症相关参数无关,乳酸浓度较高(≥4 mmol/L vs≤2 mmol/L)的患者ICU入院率(51% vs 24%)和住院死亡率(44% vs 14%)较高。结论:社区急诊科的就诊时间、抽乳酸时间、抗生素时间和液体复苏均可提高。未来的质量改进干预措施需要优化脓毒症患者的管理。乳酸浓度升高也与ICU住院率和住院死亡率独立相关。


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


