Lynn Robertson, Dolapo Ayansina, Marjorie Johnston, Angharad Marks, Corri Black
{"title":"Urban-rural and socioeconomic status: Impact on multimorbidity prevalence in hospitalized patients.","authors":"Lynn Robertson, Dolapo Ayansina, Marjorie Johnston, Angharad Marks, Corri Black","doi":"10.1177/2235042X19893470","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The aim of this study was to describe multimorbidity prevalence in hospitalized adults, by urban-rural area of residence and socioeconomic status (SES).</p><p><strong>Methods: </strong>Linked hospital episode data were used. Adults (≥18 years) admitted to hospital as an inpatient during 2014 in Grampian, Scotland, were included. Conditions were identified from admissions during the 5 years prior to the first admission in 2014. Multimorbidity was defined as ≥2 conditions and measured using Tonelli et al. based on International Classification of Diseases-10 coding (preselected list of 30 conditions). We used proportions and 95% confidence intervals (CIs) to summarize the prevalence of multimorbidity by age group, sex, urban-rural category and deprivation. The association between multimorbidity and patient characteristics was assessed using the <i>χ</i> <sup>2</sup> test.</p><p><strong>Results: </strong>Forty one thousand five hundred and forty-five patients were included (median age 62, 52.6% female). Overall, 27.4% (95% CI 27.0, 27.8) of patients were multimorbid. Multimorbidity prevalence was 28.8% (95% CI 28.1, 29.5) in large urban versus 22.0% (95% CI 20.9, 23.3) in remote rural areas and 28.7% (95% CI 27.2, 30.3) in the most deprived versus 26.0% (95% CI 25.2, 26.9) in the least deprived areas. This effect was consistent in all age groups, but not statistically significant in the age group 18-29 years. Multimorbidity increased with age but was similar for males and females.</p><p><strong>Conclusion: </strong>Given the scarcity of research into the effect of urban-rural area and SES on multimorbidity prevalence among hospitalized patients, these findings should inform future research into new models of care, including the consideration of urban-rural area and SES.</p>","PeriodicalId":92071,"journal":{"name":"Journal of comorbidity","volume":"10 ","pages":"2235042X19893470"},"PeriodicalIF":0.0000,"publicationDate":"2020-04-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ea/06/10.1177_2235042X19893470.PMC7171988.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of comorbidity","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2235042X19893470","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: The aim of this study was to describe multimorbidity prevalence in hospitalized adults, by urban-rural area of residence and socioeconomic status (SES).
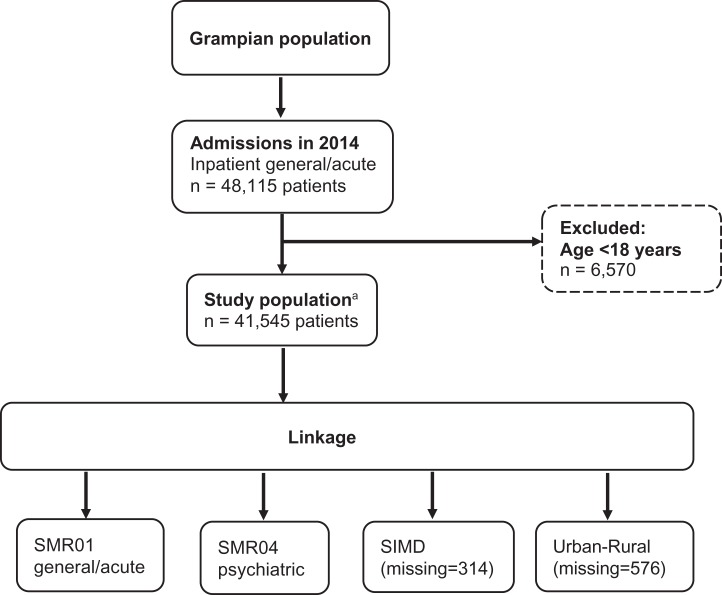
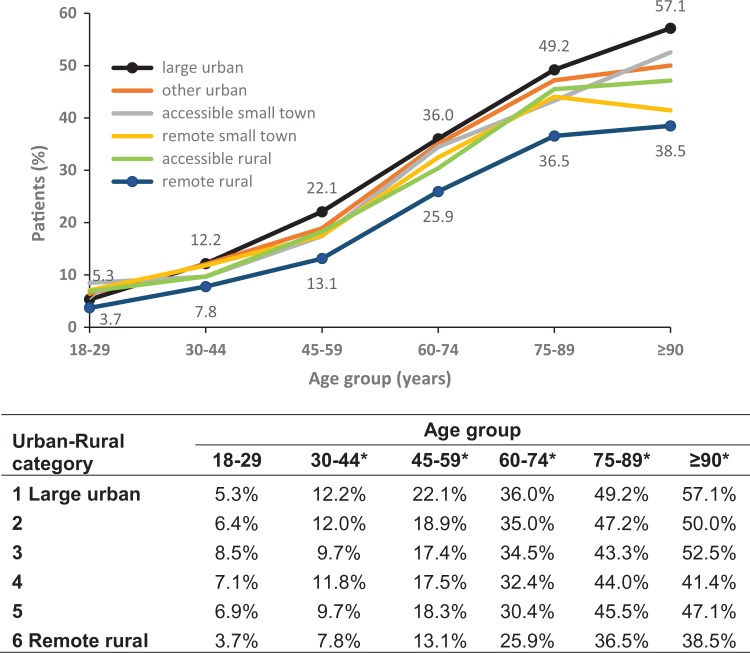
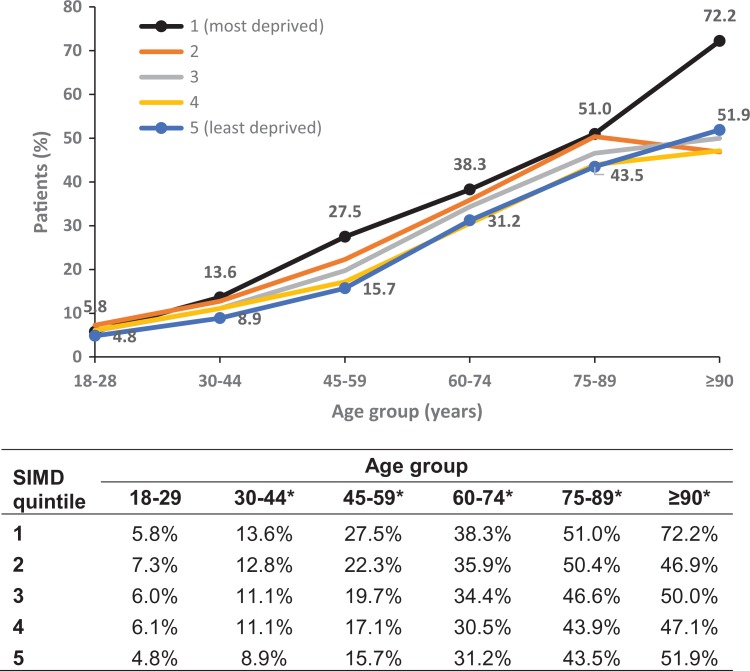
Methods: Linked hospital episode data were used. Adults (≥18 years) admitted to hospital as an inpatient during 2014 in Grampian, Scotland, were included. Conditions were identified from admissions during the 5 years prior to the first admission in 2014. Multimorbidity was defined as ≥2 conditions and measured using Tonelli et al. based on International Classification of Diseases-10 coding (preselected list of 30 conditions). We used proportions and 95% confidence intervals (CIs) to summarize the prevalence of multimorbidity by age group, sex, urban-rural category and deprivation. The association between multimorbidity and patient characteristics was assessed using the χ2 test.
Results: Forty one thousand five hundred and forty-five patients were included (median age 62, 52.6% female). Overall, 27.4% (95% CI 27.0, 27.8) of patients were multimorbid. Multimorbidity prevalence was 28.8% (95% CI 28.1, 29.5) in large urban versus 22.0% (95% CI 20.9, 23.3) in remote rural areas and 28.7% (95% CI 27.2, 30.3) in the most deprived versus 26.0% (95% CI 25.2, 26.9) in the least deprived areas. This effect was consistent in all age groups, but not statistically significant in the age group 18-29 years. Multimorbidity increased with age but was similar for males and females.
Conclusion: Given the scarcity of research into the effect of urban-rural area and SES on multimorbidity prevalence among hospitalized patients, these findings should inform future research into new models of care, including the consideration of urban-rural area and SES.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


