Long-term persistence and adherence with non-vitamin K oral anticoagulants in patients with atrial fibrillation and their associations with stroke risk.
Joris J Komen, Eibert R Heerdink, Olaf H Klungel, Aukje K Mantel-Teeuwisse, Tomas Forslund, Björn Wettermark, Paul Hjemdahl
{"title":"Long-term persistence and adherence with non-vitamin K oral anticoagulants in patients with atrial fibrillation and their associations with stroke risk.","authors":"Joris J Komen, Eibert R Heerdink, Olaf H Klungel, Aukje K Mantel-Teeuwisse, Tomas Forslund, Björn Wettermark, Paul Hjemdahl","doi":"10.1093/ehjcvp/pvaa017","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Studies on adherence and persistence with non-vitamin K oral anticoagulant (NOAC) treatment have relied on data from the early years of NOAC availability. We aimed to study long-term adherence and persistence with NOACs and their association with stroke risk.</p><p><strong>Methods and results: </strong>From the Stockholm Healthcare database, we included 21 028 atrial fibrillation patients claiming a first NOAC prescription from July 2011 until October 2018, with more than 1000 patients having more than 5 years of follow-up (median: 2.0, interquartile range: 1.0-3.2). Persistence rates, defined as continuing to claim NOAC prescriptions within a 90-day gap, decreased to 70% at the end of follow-up. However, 85% of the patients were treated at the end of the study due to reinitiations. Adherence, calculated as medication possession rate (MPR) in 3 and 6-month intervals among persistent users, remained stable at 90%, with 75% of patients having an MPR >95% throughout the study period. Using a case-control design, we calculated associations of persistence and adherence with stroke risk, adjusting for potential confounders. The outcome was a composite of ischaemic or unspecified stroke and transient ischaemic attack. Non-persistence and poor adherence were both associated with increased stroke risk [non-persistence adjusted odds ratio (aOR): 2.05; 95% confidence interval (CI): 1.49-2.82, 1% reduction MPR aOR: 1.03; CI: 1.01-1.05]. There was no association between non-persistence or poor adherence and the falsification endpoints; fractions and respiratory infections, indicating no 'healthy-adherer' effect.</p><p><strong>Conclusion: </strong>Persistence rates decreased slowly over time, but persistent patients had high adherence rates. Both non-persistence and poor adherence were associated with an increased stroke risk.</p>","PeriodicalId":11995,"journal":{"name":"European Heart Journal — Cardiovascular Pharmacotherapy","volume":" ","pages":"f72-f80"},"PeriodicalIF":0.0000,"publicationDate":"2021-04-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1093/ehjcvp/pvaa017","citationCount":"30","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal — Cardiovascular Pharmacotherapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ehjcvp/pvaa017","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 30
Abstract
Aims: Studies on adherence and persistence with non-vitamin K oral anticoagulant (NOAC) treatment have relied on data from the early years of NOAC availability. We aimed to study long-term adherence and persistence with NOACs and their association with stroke risk.
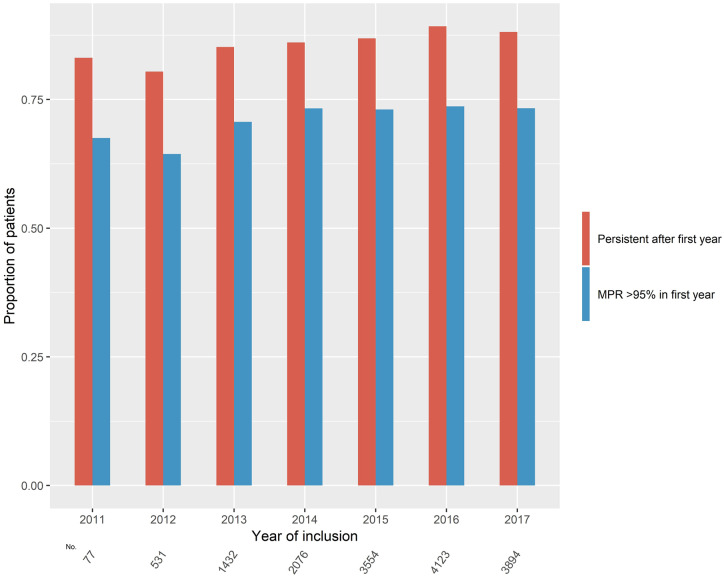
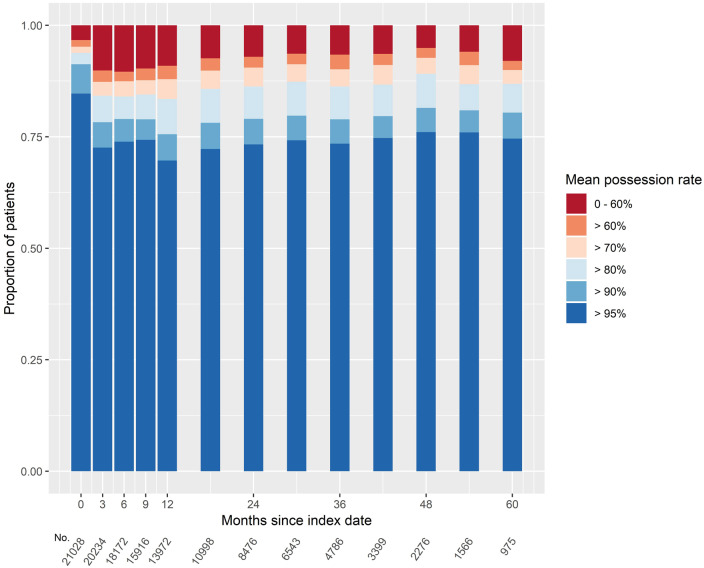
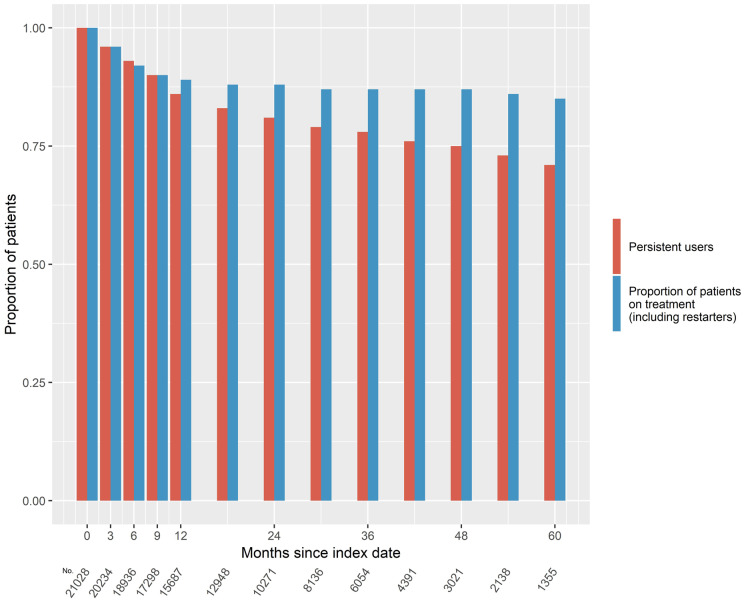
Methods and results: From the Stockholm Healthcare database, we included 21 028 atrial fibrillation patients claiming a first NOAC prescription from July 2011 until October 2018, with more than 1000 patients having more than 5 years of follow-up (median: 2.0, interquartile range: 1.0-3.2). Persistence rates, defined as continuing to claim NOAC prescriptions within a 90-day gap, decreased to 70% at the end of follow-up. However, 85% of the patients were treated at the end of the study due to reinitiations. Adherence, calculated as medication possession rate (MPR) in 3 and 6-month intervals among persistent users, remained stable at 90%, with 75% of patients having an MPR >95% throughout the study period. Using a case-control design, we calculated associations of persistence and adherence with stroke risk, adjusting for potential confounders. The outcome was a composite of ischaemic or unspecified stroke and transient ischaemic attack. Non-persistence and poor adherence were both associated with increased stroke risk [non-persistence adjusted odds ratio (aOR): 2.05; 95% confidence interval (CI): 1.49-2.82, 1% reduction MPR aOR: 1.03; CI: 1.01-1.05]. There was no association between non-persistence or poor adherence and the falsification endpoints; fractions and respiratory infections, indicating no 'healthy-adherer' effect.
Conclusion: Persistence rates decreased slowly over time, but persistent patients had high adherence rates. Both non-persistence and poor adherence were associated with an increased stroke risk.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


