Generalist versus Abdominal Subspecialist Radiologist Interpretations of Abdominopelvic Computed Tomography Performed on Patients with Abdominal Pain and its Impact on the Therapeutic Approach.
Hasan Yesilagac, Ilker Murat Arer, Betul Gulalp, Hakan Yabanoglu, Ozlem Karagun, Elif Karadeli
{"title":"Generalist versus Abdominal Subspecialist Radiologist Interpretations of Abdominopelvic Computed Tomography Performed on Patients with Abdominal Pain and its Impact on the Therapeutic Approach.","authors":"Hasan Yesilagac, Ilker Murat Arer, Betul Gulalp, Hakan Yabanoglu, Ozlem Karagun, Elif Karadeli","doi":"10.22114/ajem.v0i0.288","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Abdominal pain is one of the most common patient complaints in the emergency department (ED) and abdominopelvic computed tomography (ACT) scan plays an important role in evaluation of these patients.</p><p><strong>Objective: </strong>The aim of this study was to determine the differences between interpretations by generalist radiologists and abdominal subspecialist radiologists regarding the abdominopelvic computed tomography (ACT) of patients who were admitted to the Emergency Department (ED) and to investigate its effect on the patients' therapeutic approach.</p><p><strong>Methods: </strong>The records of 16452 patients who were admitted to the emergency department with complaint of abdominal pain between January 2015 and April 2017 were reviewed, retrospectively. Out of these patients, 245 (1.5%) underwent ACT for differential diagnosis and among them, 137 (0.8%) patients had their ACT reports evaluated by generalist radiologists in 45 minutes and by abdominal subspecialist radiologist 8-12 hours later and were included in the study. Patients were divided into three groups according to the effect of ACT reports on the performed treatment. Group 1: no effect on planned treatment, group 2: minor effect on planned treatment, which did not result in a change in the treatment process and group 3: major effect on planned treatment approach, which resulted in a change in the treatment process. These changes included at least one of the two criteria: changing the indication of surgery from emergency surgery to elective surgery and/or discharge of the patient from the ED, when actually hospitalization was required.</p><p><strong>Results: </strong>Out of the 137 patients, 87 (63.5%) were male, 50 (36.5%) were female and the patients' mean age was 56 (27-93) years. There were 117 (85.4%) patients in group 1, 15 (10.9%) patients in group 2, and 5 (3.7%) patients in group 3. We determined minor inconsistency between the reports in group 2 and major inconsistency in group 3. Patients in group 3 suffered from delayed surgical intervention due to inconsistency of the CT reports resulting in prolonged hospital stay and increased morbidity. In 17 patients (four patients in Group 1 and 13 patients in Group 2) treatment plan was changed due to CT results; and while surgical treatment was planned for them prior to CT scan, they were discharged with medical treatment after that and overtreatment was prevented.</p><p><strong>Conclusion: </strong>Contribution of abdominal radiologists to evaluation of ACT images in the ED would reduce the inconsistency in ACT reports and prevent the patients from receiving insufficient treatment or overtreatment.</p>","PeriodicalId":7290,"journal":{"name":"Advanced Journal of Emergency Medicine","volume":"4 2","pages":"e21"},"PeriodicalIF":0.0000,"publicationDate":"2020-01-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/cb/c3/AJEM-4-e21.PMC7163262.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advanced Journal of Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22114/ajem.v0i0.288","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Abdominal pain is one of the most common patient complaints in the emergency department (ED) and abdominopelvic computed tomography (ACT) scan plays an important role in evaluation of these patients.
Objective: The aim of this study was to determine the differences between interpretations by generalist radiologists and abdominal subspecialist radiologists regarding the abdominopelvic computed tomography (ACT) of patients who were admitted to the Emergency Department (ED) and to investigate its effect on the patients' therapeutic approach.
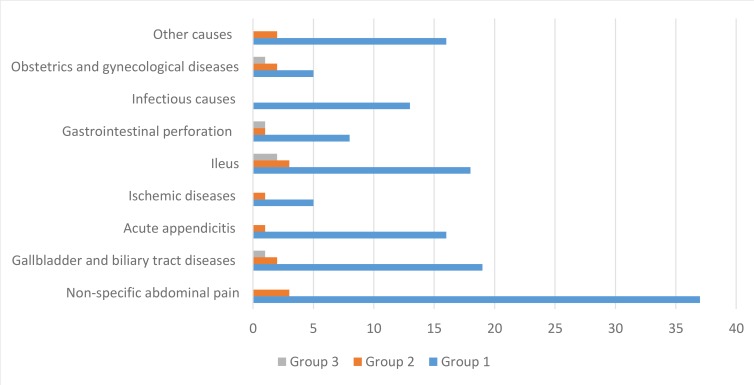
Methods: The records of 16452 patients who were admitted to the emergency department with complaint of abdominal pain between January 2015 and April 2017 were reviewed, retrospectively. Out of these patients, 245 (1.5%) underwent ACT for differential diagnosis and among them, 137 (0.8%) patients had their ACT reports evaluated by generalist radiologists in 45 minutes and by abdominal subspecialist radiologist 8-12 hours later and were included in the study. Patients were divided into three groups according to the effect of ACT reports on the performed treatment. Group 1: no effect on planned treatment, group 2: minor effect on planned treatment, which did not result in a change in the treatment process and group 3: major effect on planned treatment approach, which resulted in a change in the treatment process. These changes included at least one of the two criteria: changing the indication of surgery from emergency surgery to elective surgery and/or discharge of the patient from the ED, when actually hospitalization was required.
Results: Out of the 137 patients, 87 (63.5%) were male, 50 (36.5%) were female and the patients' mean age was 56 (27-93) years. There were 117 (85.4%) patients in group 1, 15 (10.9%) patients in group 2, and 5 (3.7%) patients in group 3. We determined minor inconsistency between the reports in group 2 and major inconsistency in group 3. Patients in group 3 suffered from delayed surgical intervention due to inconsistency of the CT reports resulting in prolonged hospital stay and increased morbidity. In 17 patients (four patients in Group 1 and 13 patients in Group 2) treatment plan was changed due to CT results; and while surgical treatment was planned for them prior to CT scan, they were discharged with medical treatment after that and overtreatment was prevented.
Conclusion: Contribution of abdominal radiologists to evaluation of ACT images in the ED would reduce the inconsistency in ACT reports and prevent the patients from receiving insufficient treatment or overtreatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


