The Impact of an Attending Intensivist on the Clinical Outcomes of Patients Admitted to the Cardiac Surgical Intensive Care Unit after Coronary Artery Bypass Grafting.
Dong Jung Kim, Bongyeon Sohn, Hakju Kim, Hyoung Woo Chang, Jae Hang Lee, Jun Sung Kim, Cheong Lim, Kay-Hyun Park
{"title":"The Impact of an Attending Intensivist on the Clinical Outcomes of Patients Admitted to the Cardiac Surgical Intensive Care Unit after Coronary Artery Bypass Grafting.","authors":"Dong Jung Kim, Bongyeon Sohn, Hakju Kim, Hyoung Woo Chang, Jae Hang Lee, Jun Sung Kim, Cheong Lim, Kay-Hyun Park","doi":"10.5090/kjtcs.2020.53.1.8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>We aimed to investigate the associations of critical care provided in a cardiac surgical intensive care unit (CSICU) staffed by an attending intensivist with improvements in intensive care unit (ICU) quality and reductions in postoperative complications.</p><p><strong>Methods: </strong>Patients who underwent elective isolated coronary artery bypass grafting (CABG) between January 2007 and December 2012 (the control group) were propensity-matched (1:1) to CABG patients between January 2013 and June 2018 (the intensivist group).</p><p><strong>Results: </strong>Using propensity score matching, 302 patients were extracted from each group. The proportion of patients with at least 1 postoperative complication was significantly lower in the intensivist group than in the control group (17.2% vs. 28.5%, p=0.001). In the intensivist group, the duration of mechanical ventilation (6.4±13.7 hours vs. 13.7±49.3 hours, p=0.013) and length of ICU stay (28.7±33.9 hours vs. 41.7±90.4 hours, p=0.018) were significantly shorter than in the control group. The proportions of patients with prolonged mechanical ventilation (2.3% vs. 7.6%, p=0.006), delirium (1.3% vs. 6.3%, p=0.003) and acute kidney injury (1.3% vs. 5.3%, p=0.012) were significantly lower in the intensivist group than in the control group.</p><p><strong>Conclusion: </strong>A transition from an open ICU model with trainee coverage to a closed ICU model with attending intensivist coverage can be expected to yield improvements in CSICU quality and reductions in postoperative complications.</p>","PeriodicalId":38678,"journal":{"name":"Korean Journal of Thoracic and Cardiovascular Surgery","volume":"53 1","pages":"8-15"},"PeriodicalIF":0.0000,"publicationDate":"2020-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ee/e8/kjtcv-53-008.PMC7006613.pdf","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Thoracic and Cardiovascular Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5090/kjtcs.2020.53.1.8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/2/5 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 3
Abstract
Background: We aimed to investigate the associations of critical care provided in a cardiac surgical intensive care unit (CSICU) staffed by an attending intensivist with improvements in intensive care unit (ICU) quality and reductions in postoperative complications.
Methods: Patients who underwent elective isolated coronary artery bypass grafting (CABG) between January 2007 and December 2012 (the control group) were propensity-matched (1:1) to CABG patients between January 2013 and June 2018 (the intensivist group).
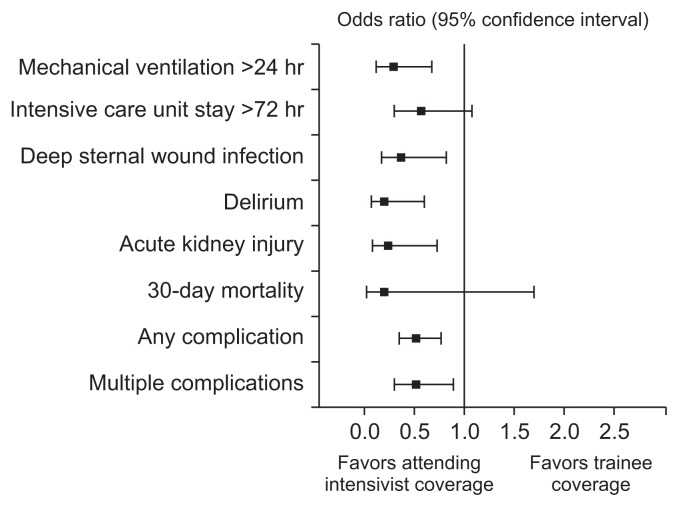
Results: Using propensity score matching, 302 patients were extracted from each group. The proportion of patients with at least 1 postoperative complication was significantly lower in the intensivist group than in the control group (17.2% vs. 28.5%, p=0.001). In the intensivist group, the duration of mechanical ventilation (6.4±13.7 hours vs. 13.7±49.3 hours, p=0.013) and length of ICU stay (28.7±33.9 hours vs. 41.7±90.4 hours, p=0.018) were significantly shorter than in the control group. The proportions of patients with prolonged mechanical ventilation (2.3% vs. 7.6%, p=0.006), delirium (1.3% vs. 6.3%, p=0.003) and acute kidney injury (1.3% vs. 5.3%, p=0.012) were significantly lower in the intensivist group than in the control group.
Conclusion: A transition from an open ICU model with trainee coverage to a closed ICU model with attending intensivist coverage can be expected to yield improvements in CSICU quality and reductions in postoperative complications.
背景:我们的目的是调查在心脏外科重症监护病房(CSICU)提供的重症监护与重症监护病房(ICU)质量的改善和术后并发症的减少之间的关系。方法:2007年1月至2012年12月期间行选择性孤立冠状动脉旁路移植术(CABG)的患者(对照组)与2013年1月至2018年6月期间行CABG的患者(强化治疗组)倾向匹配(1:1)。结果:采用倾向评分匹配法,每组抽取302例患者。强化治疗组出现至少1例术后并发症的患者比例明显低于对照组(17.2% vs. 28.5%, p=0.001)。重症监护组机械通气时间(6.4±13.7 h比13.7±49.3 h, p=0.013)和ICU住院时间(28.7±33.9 h比41.7±90.4 h, p=0.018)均显著短于对照组。强化组延长机械通气时间(2.3% vs. 7.6%, p=0.006)、谵妄(1.3% vs. 6.3%, p=0.003)、急性肾损伤(1.3% vs. 5.3%, p=0.012)的比例均显著低于对照组。结论:从有培训生覆盖的开放式ICU模式过渡到有主治重症医师覆盖的封闭式ICU模式,有望提高CSICU质量,减少术后并发症。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


