John Barnard, Tyler Overholt, Ali Hajiran, Chad Crigger, Morris Jessop, Jennifer Knight, Chad Morley
{"title":"Traumatic Bladder Ruptures: A Ten-Year Review at a Level 1 Trauma Center.","authors":"John Barnard, Tyler Overholt, Ali Hajiran, Chad Crigger, Morris Jessop, Jennifer Knight, Chad Morley","doi":"10.1155/2019/2614586","DOIUrl":null,"url":null,"abstract":"<p><p>Bladder rupture occurs in only 1.6% of blunt abdominopelvic trauma cases. Although rare, bladder rupture can result in significant morbidity if undiagnosed or inappropriately managed. AUA Urotrauma Guidelines suggest that urethral catheter drainage is a standard of care for both extraperitoneal and intraperitoneal bladder rupture regardless of the need for surgical repair. However, no specific guidance is given regarding the length of catheterization. The present study seeks to summarize contemporary management of bladder trauma at our tertiary care center, assess the impact of length of catheterization on bladder injuries and complications, and develop a protocol for management of bladder injuries from time of injury to catheter removal. A retrospective review was performed on 34,413 blunt trauma cases to identify traumatic bladder ruptures over the past 10 years (January 2008-January 2018) at our tertiary care facility. Patient data were collected including age, gender, BMI, mechanism of injury, and type of injury. The primary treatment modality (surgical repair vs. catheter drainage only), length of catheterization, and post-injury complications were also assessed. Review of our institutional trauma database identified 44 patients with bladder trauma. Mean age was 41 years, mean BMI was 24.8 kg/m<sup>2</sup>, 95% were Caucasian, and 55% were female. Motor vehicle collision (MVC) was the most common mechanism, representing 45% of total injuries. Other mechanisms included falls (20%) and all-terrain vehicle (ATV) accidents (13.6%). 31 patients had extraperitoneal injury, and 13 were intraperitoneal. Pelvic fractures were present in 93%, and 39% had additional solid organ injuries. Formal cystogram was performed in 59% on presentation, and mean time to cystogram was 4 hours. Gross hematuria was noted in 95% of cases. Operative management was performed for all intraperitoneal injuries and 35.5% of extraperitoneal cases. Bladder closure in operative cases was typically performed in 2 layers with absorbable suture in a running fashion. The intraperitoneal and extraperitoneal injuries managed operatively were compared, and length of catheterization (28 d vs. 22 d, <i>p</i>=0.46), time from injury to normal fluorocystogram (19.8 d vs. 20.7 d, <i>p</i>=0.80), and time from injury to repair (4.3 vs. 60.5 h, <i>p</i>=0.23) were not statistically different between cohorts. Patients whose catheter remained in place for greater than 14 days had prolonged time to initial cystogram (26.6 d vs. 11.5 d) compared with those whose foley catheter was removed within 14 days. The complication rate was 21% for catheters left more than 14 days while patients whose catheter remained less than 14 days experienced no complications. The present study provides a 10-year retrospective review characterizing the presentation, management, and follow-up of bladder trauma patients at our level 1 trauma center. Based on our findings, we have developed an institutional protocol which now includes recommendations regarding length of catheterization after traumatic bladder rupture. By providing specific guidelines for initial follow-up cystogram and foley removal, we hope to decrease patient morbidity from prolonged catheterization. Further study will seek to allow multidisciplinary trauma teams to standardize management, streamline care, and minimize complications for patients presenting with traumatic bladder injuries.</p>","PeriodicalId":7490,"journal":{"name":"Advances in Urology","volume":"2019 ","pages":"2614586"},"PeriodicalIF":2.3000,"publicationDate":"2019-12-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6930775/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2019/2614586","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
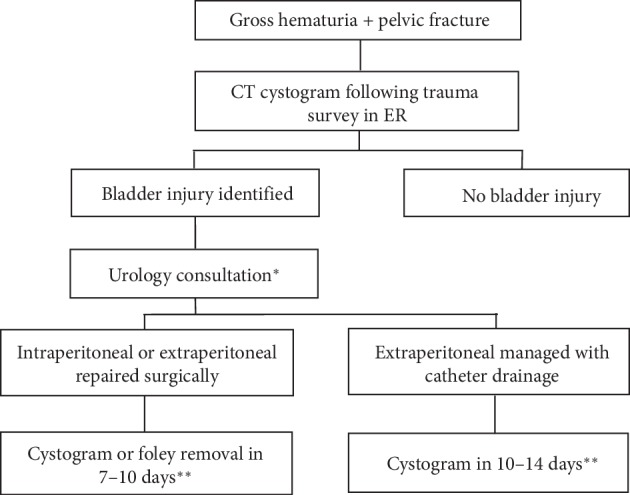
Bladder rupture occurs in only 1.6% of blunt abdominopelvic trauma cases. Although rare, bladder rupture can result in significant morbidity if undiagnosed or inappropriately managed. AUA Urotrauma Guidelines suggest that urethral catheter drainage is a standard of care for both extraperitoneal and intraperitoneal bladder rupture regardless of the need for surgical repair. However, no specific guidance is given regarding the length of catheterization. The present study seeks to summarize contemporary management of bladder trauma at our tertiary care center, assess the impact of length of catheterization on bladder injuries and complications, and develop a protocol for management of bladder injuries from time of injury to catheter removal. A retrospective review was performed on 34,413 blunt trauma cases to identify traumatic bladder ruptures over the past 10 years (January 2008-January 2018) at our tertiary care facility. Patient data were collected including age, gender, BMI, mechanism of injury, and type of injury. The primary treatment modality (surgical repair vs. catheter drainage only), length of catheterization, and post-injury complications were also assessed. Review of our institutional trauma database identified 44 patients with bladder trauma. Mean age was 41 years, mean BMI was 24.8 kg/m2, 95% were Caucasian, and 55% were female. Motor vehicle collision (MVC) was the most common mechanism, representing 45% of total injuries. Other mechanisms included falls (20%) and all-terrain vehicle (ATV) accidents (13.6%). 31 patients had extraperitoneal injury, and 13 were intraperitoneal. Pelvic fractures were present in 93%, and 39% had additional solid organ injuries. Formal cystogram was performed in 59% on presentation, and mean time to cystogram was 4 hours. Gross hematuria was noted in 95% of cases. Operative management was performed for all intraperitoneal injuries and 35.5% of extraperitoneal cases. Bladder closure in operative cases was typically performed in 2 layers with absorbable suture in a running fashion. The intraperitoneal and extraperitoneal injuries managed operatively were compared, and length of catheterization (28 d vs. 22 d, p=0.46), time from injury to normal fluorocystogram (19.8 d vs. 20.7 d, p=0.80), and time from injury to repair (4.3 vs. 60.5 h, p=0.23) were not statistically different between cohorts. Patients whose catheter remained in place for greater than 14 days had prolonged time to initial cystogram (26.6 d vs. 11.5 d) compared with those whose foley catheter was removed within 14 days. The complication rate was 21% for catheters left more than 14 days while patients whose catheter remained less than 14 days experienced no complications. The present study provides a 10-year retrospective review characterizing the presentation, management, and follow-up of bladder trauma patients at our level 1 trauma center. Based on our findings, we have developed an institutional protocol which now includes recommendations regarding length of catheterization after traumatic bladder rupture. By providing specific guidelines for initial follow-up cystogram and foley removal, we hope to decrease patient morbidity from prolonged catheterization. Further study will seek to allow multidisciplinary trauma teams to standardize management, streamline care, and minimize complications for patients presenting with traumatic bladder injuries.
期刊介绍:
Advances in Urology is a peer-reviewed, open access journal that publishes state-of-the-art reviews and original research papers of wide interest in all fields of urology. The journal strives to provide publication of important manuscripts to the widest possible audience worldwide, without the constraints of expensive, hard-to-access, traditional bound journals. Advances in Urology is designed to improve publication access of both well-established urologic scientists and less well-established writers, by allowing interested scientists worldwide to participate fully.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


