Increased blood pressure variability after acute ischemic stroke increases the risk of death: A secondary analysis of the Virtual International Stroke Trial Archive.
Adam de Havenon, Greg Stoddard, Monica Saini, Ka-Ho Wong, David Tirschwell, Phillip Bath
{"title":"Increased blood pressure variability after acute ischemic stroke increases the risk of death: A secondary analysis of the Virtual International Stroke Trial Archive.","authors":"Adam de Havenon, Greg Stoddard, Monica Saini, Ka-Ho Wong, David Tirschwell, Phillip Bath","doi":"10.1177/2048004019856496","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Despite promising epidemiological data, it remains unclear if increased blood pressure variability is associated with death after acute ischemic stroke. Our objective was to examine this association in a large cohort of acute ischemic stroke patients.</p><p><strong>Methods: </strong>We conducted a retrospective analysis of anonymized, pooled, participant data from the Virtual International Stroke Trial Archive. We included patients with a 90-day modified Rankin Scale and blood pressure readings in the 24 h after study enrollment. The exposure was blood pressure variability during the day after study enrollment, calculated for the systolic and diastolic blood pressure using six statistical methodologies. The primary outcome was death within 90 days of stroke onset.</p><p><strong>Results: </strong>Our cohort comprised 1891 patients of whom 277 (14.7%) died within 90 days. All indices of blood pressure variability were higher in patients who died, but the difference was more pronounced for systolic than diastolic blood pressure variability (systolic standard deviation for alive versus dead patients = 13.4 versus 15.9 mmHg, p < 0.001). Similar results were found in logistic regression models fit to the outcome of death, but only systolic blood pressure variability remained significant in adjusted models (Odds Ratio for death when comparing highest to lowest tercile of systolic blood pressure variability = 1.41-1.89, p < 0.03 for all).<b>Conclusions and relevance:</b> These results reinforce prior studies that found increased blood pressure variability is associated with worse neurologic outcome after stroke. These data should help guide research on blood pressure variability after stroke and advocate for the inclusion of death as a clinical outcome in future studies that therapeutically reduce blood pressure variability.</p>","PeriodicalId":30457,"journal":{"name":"JRSM Cardiovascular Disease","volume":"8 ","pages":"2048004019856496"},"PeriodicalIF":1.4000,"publicationDate":"2019-06-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/2048004019856496","citationCount":"15","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JRSM Cardiovascular Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2048004019856496","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 15
Abstract
Background: Despite promising epidemiological data, it remains unclear if increased blood pressure variability is associated with death after acute ischemic stroke. Our objective was to examine this association in a large cohort of acute ischemic stroke patients.
Methods: We conducted a retrospective analysis of anonymized, pooled, participant data from the Virtual International Stroke Trial Archive. We included patients with a 90-day modified Rankin Scale and blood pressure readings in the 24 h after study enrollment. The exposure was blood pressure variability during the day after study enrollment, calculated for the systolic and diastolic blood pressure using six statistical methodologies. The primary outcome was death within 90 days of stroke onset.
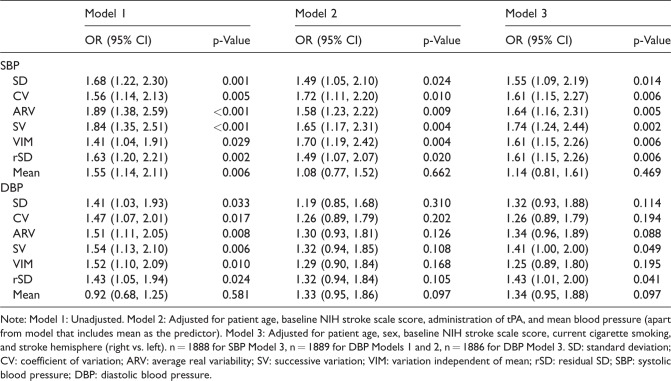
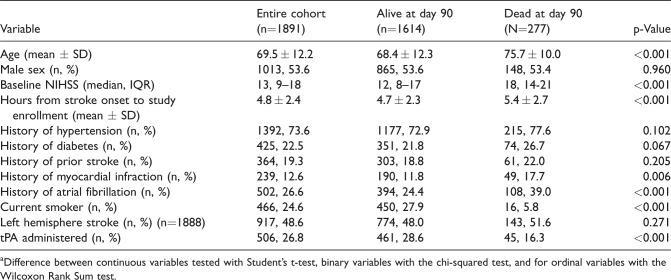
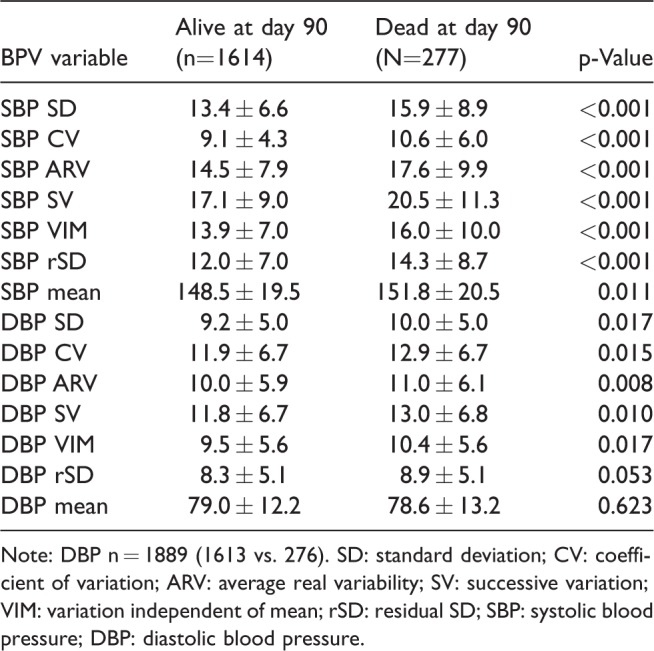
Results: Our cohort comprised 1891 patients of whom 277 (14.7%) died within 90 days. All indices of blood pressure variability were higher in patients who died, but the difference was more pronounced for systolic than diastolic blood pressure variability (systolic standard deviation for alive versus dead patients = 13.4 versus 15.9 mmHg, p < 0.001). Similar results were found in logistic regression models fit to the outcome of death, but only systolic blood pressure variability remained significant in adjusted models (Odds Ratio for death when comparing highest to lowest tercile of systolic blood pressure variability = 1.41-1.89, p < 0.03 for all).Conclusions and relevance: These results reinforce prior studies that found increased blood pressure variability is associated with worse neurologic outcome after stroke. These data should help guide research on blood pressure variability after stroke and advocate for the inclusion of death as a clinical outcome in future studies that therapeutically reduce blood pressure variability.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


