Mei Sian Fu, Soo Jin Lim, Maisarah Jalalonmuhali, Kee Seong Ng, Soo Kun Lim, Kok Peng Ng
{"title":"Clinical Significance of Renal Allograft Protocol Biopsies: A Single Tertiary Center Experience in Malaysia.","authors":"Mei Sian Fu, Soo Jin Lim, Maisarah Jalalonmuhali, Kee Seong Ng, Soo Kun Lim, Kok Peng Ng","doi":"10.1155/2019/9153875","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The role of protocol renal allograft biopsy in kidney transplantation is controversial due to the concern with procedural-related complications; however, its role is slowly evolving. Recent evidence suggests that protocol biopsy is useful in detecting subclinical renal pathology. Early recognition and treatment of renal pathologies can improve long-term outcomes of renal allografts.</p><p><strong>Methodology: </strong>A total of 362 renal allograft protocol biopsies were performed in adult recipients of kidney transplantation between 2012 and 2017. After excluding those with poor quality or those performed with a baseline serum creatinine level >200 umol/L, we analyzed 334 (92.3%) biopsies. Histology reports were reviewed and categorized into histoimmunological and nonimmunological changes. The immunological changes were subcategorized into the following: (1) no acute rejection (NR), (2) borderline changes (BC), and (3) subclinical rejection (SCR). Nonimmunological changes were subcategorized into the following: (1) chronicity including interstitial fibrosis/tubular atrophy (IFTA), chronic T-cell-mediated rejection (TCMR), unspecified chronic lesions, and arterionephrosclerosis, (2) de novo glomerulopathy/recurrence of primary disease (RP), and (3) other clinically unsuspected lesions (acute pyelonephritis, calcineurin inhibitors toxicity, postinfective glomerulonephritis, and BK virus nephropathy). Risk factors associated with SCR were assessed.</p><p><strong>Results: </strong>For the histoimmunological changes, 161 (48.2%) showed NR, 145 (43.4%) were BC, and 28 (8.4%) were SCR. These clinical events were more pronounced for the first 5 years; our data showed BC accounted for 59 (36.4%), 64 (54.2%), and 22 (40.7%) biopsies within <1 year, 1-5 years, and > 5 years, respectively (p = 0.011). Meanwhile, the incidence for SCR was 6 (3.7%) biopsies in <1 year, 18 (15.3%) in 1-5 years, and 4 (7.4%) in >5 years after transplantation (p=0.003). For the nonimmunological changes, chronicity, de novo glomerulopathy/RP, and other clinically unsuspected lesions were seen in 40 (12%), 10 (3%), and 12 (3.6%) biopsies, respectively. Living-related donor recipients were associated with decreased SCR (p=0.007).</p><p><strong>Conclusions: </strong>Despite having a stable renal function, our transplant recipients had a significant number of subclinical rejection on renal allograft biopsies.</p>","PeriodicalId":45795,"journal":{"name":"Journal of Transplantation","volume":"2019 ","pages":"9153875"},"PeriodicalIF":2.2000,"publicationDate":"2019-05-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2019/9153875","citationCount":"7","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Transplantation","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2019/9153875","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 7
Abstract
Background: The role of protocol renal allograft biopsy in kidney transplantation is controversial due to the concern with procedural-related complications; however, its role is slowly evolving. Recent evidence suggests that protocol biopsy is useful in detecting subclinical renal pathology. Early recognition and treatment of renal pathologies can improve long-term outcomes of renal allografts.
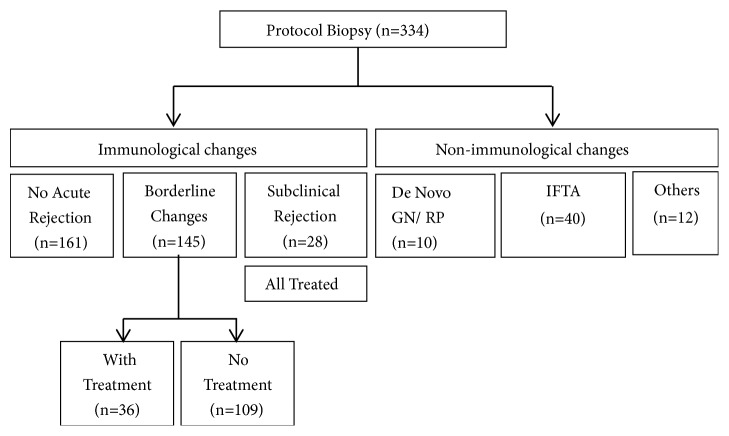
Methodology: A total of 362 renal allograft protocol biopsies were performed in adult recipients of kidney transplantation between 2012 and 2017. After excluding those with poor quality or those performed with a baseline serum creatinine level >200 umol/L, we analyzed 334 (92.3%) biopsies. Histology reports were reviewed and categorized into histoimmunological and nonimmunological changes. The immunological changes were subcategorized into the following: (1) no acute rejection (NR), (2) borderline changes (BC), and (3) subclinical rejection (SCR). Nonimmunological changes were subcategorized into the following: (1) chronicity including interstitial fibrosis/tubular atrophy (IFTA), chronic T-cell-mediated rejection (TCMR), unspecified chronic lesions, and arterionephrosclerosis, (2) de novo glomerulopathy/recurrence of primary disease (RP), and (3) other clinically unsuspected lesions (acute pyelonephritis, calcineurin inhibitors toxicity, postinfective glomerulonephritis, and BK virus nephropathy). Risk factors associated with SCR were assessed.
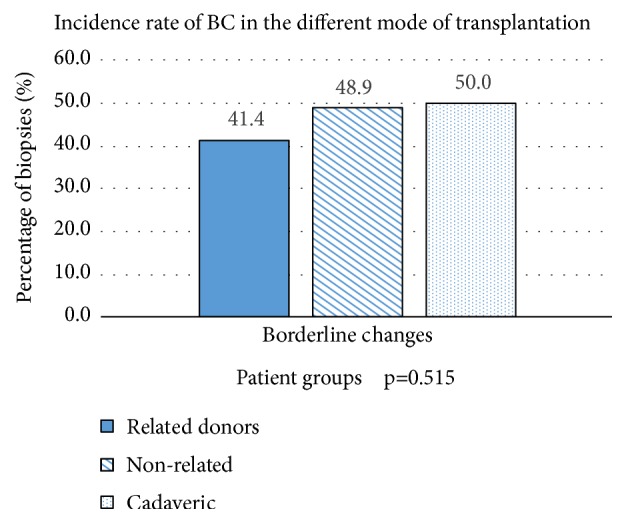
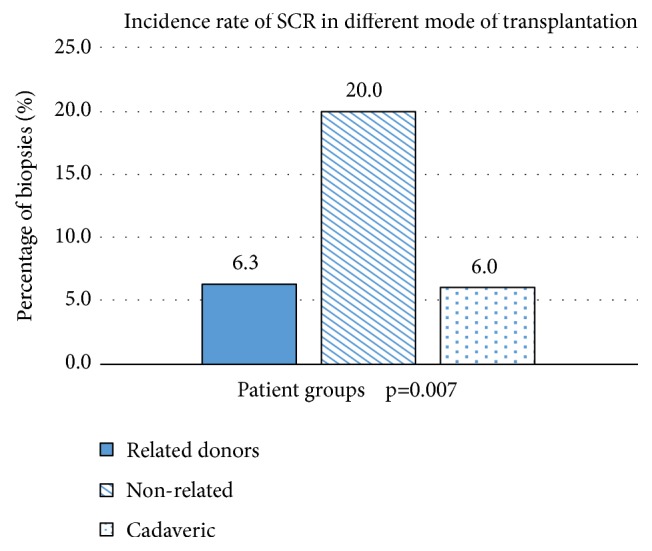
Results: For the histoimmunological changes, 161 (48.2%) showed NR, 145 (43.4%) were BC, and 28 (8.4%) were SCR. These clinical events were more pronounced for the first 5 years; our data showed BC accounted for 59 (36.4%), 64 (54.2%), and 22 (40.7%) biopsies within <1 year, 1-5 years, and > 5 years, respectively (p = 0.011). Meanwhile, the incidence for SCR was 6 (3.7%) biopsies in <1 year, 18 (15.3%) in 1-5 years, and 4 (7.4%) in >5 years after transplantation (p=0.003). For the nonimmunological changes, chronicity, de novo glomerulopathy/RP, and other clinically unsuspected lesions were seen in 40 (12%), 10 (3%), and 12 (3.6%) biopsies, respectively. Living-related donor recipients were associated with decreased SCR (p=0.007).
Conclusions: Despite having a stable renal function, our transplant recipients had a significant number of subclinical rejection on renal allograft biopsies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


