{"title":"Gastroschisis Following Treatment with High-Dose Methimazole in Pregnancy: A Case Report.","authors":"Dyah Purnamasari, Susie Setyowati, Em Yunir, Anandhara Indriani Khumaedi, Dante Saksono Harbuwono","doi":"10.1007/s40800-019-0099-2","DOIUrl":null,"url":null,"abstract":"<p><p>Hyperthyroidism in pregnancy is associated with a increased incidence of low birth weight, preterm birth and admission to the neonatal intensive care unit. However, available treatment options are limited. In this report, we present a case of fetal gastroschisis with a history of intrauterine exposure to methimazole. A 37-year-old woman was diagnosed with Grave's disease 3 years before her pregnancy. She had a poor response to propylthiouracil and required high-dose methimazole before her pregnancy. During the first trimester, she received methimazole 120 mg/day. After her 12th week of pregnancy, she received block-and-replace therapy (levothyroxine [LT4] 50 µg/day) because of the risk of hypothyroidism, and the dose of methimazole was downtitrated to 60 mg/day. Fetal ultrasonography showed fetal growth retardation and gastroschisis at gestational week 33. The relationship between the very high doses of methimazole in the first trimester of pregnancy and the incidence of gastroschisis in this patient was not fully understood because evidence of a relationship between the use of antithyroid drugs in the first trimester and congenital abnormalities in the fetus is lacking. Furthermore block-and-replace therapy is not recommended in pregnancy because it requires a higher dose of methimazole. We recommend preconception counseling and early screening of thyroid function. The counseling should include the best timeline for pregnancy and a discussion of the risks and benefits of hyperthyroidism treatment options.</p>","PeriodicalId":11364,"journal":{"name":"Drug Safety - Case Reports","volume":"6 1","pages":"5"},"PeriodicalIF":0.0000,"publicationDate":"2019-05-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1007/s40800-019-0099-2","citationCount":"7","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drug Safety - Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s40800-019-0099-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 7
Abstract
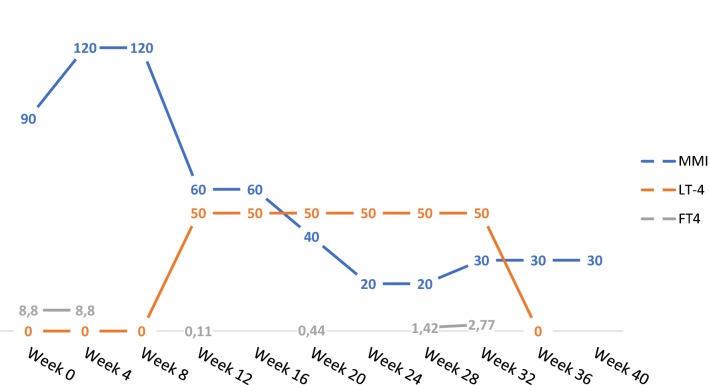
Hyperthyroidism in pregnancy is associated with a increased incidence of low birth weight, preterm birth and admission to the neonatal intensive care unit. However, available treatment options are limited. In this report, we present a case of fetal gastroschisis with a history of intrauterine exposure to methimazole. A 37-year-old woman was diagnosed with Grave's disease 3 years before her pregnancy. She had a poor response to propylthiouracil and required high-dose methimazole before her pregnancy. During the first trimester, she received methimazole 120 mg/day. After her 12th week of pregnancy, she received block-and-replace therapy (levothyroxine [LT4] 50 µg/day) because of the risk of hypothyroidism, and the dose of methimazole was downtitrated to 60 mg/day. Fetal ultrasonography showed fetal growth retardation and gastroschisis at gestational week 33. The relationship between the very high doses of methimazole in the first trimester of pregnancy and the incidence of gastroschisis in this patient was not fully understood because evidence of a relationship between the use of antithyroid drugs in the first trimester and congenital abnormalities in the fetus is lacking. Furthermore block-and-replace therapy is not recommended in pregnancy because it requires a higher dose of methimazole. We recommend preconception counseling and early screening of thyroid function. The counseling should include the best timeline for pregnancy and a discussion of the risks and benefits of hyperthyroidism treatment options.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


