Colin P Dunn, Emmanuel U Emeasoba, Ari J Holtzman, Michael Hung, Joshua Kaminetsky, Omar Alani, Stuart M Greenstein
{"title":"Comparing the Predictive Power of Preoperative Risk Assessment Tools to Best Predict Major Adverse Cardiac Events in Kidney Transplant Patients.","authors":"Colin P Dunn, Emmanuel U Emeasoba, Ari J Holtzman, Michael Hung, Joshua Kaminetsky, Omar Alani, Stuart M Greenstein","doi":"10.1155/2019/9080856","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients undergoing kidney transplantation have increased risk of adverse cardiovascular events due to histories of hypertension, end-stage renal disease, and dialysis. As such, they are especially in need of accurate preoperative risk assessment.</p><p><strong>Methods: </strong>We compared three different risk assessment models for their ability to predict major adverse cardiac events at 30 days and 1 year after transplant. These were the PORT model, the RCRI model, and the Gupta model. We used a method based on generalized U-statistics to determine statistically significant improvements in the area under the receiver operator curve (AUC), based on a common major adverse cardiac event (MACE) definition. For the top-performing model, we added new covariates into multivariable logistic regression in an attempt to create further improvement in the AUC.</p><p><strong>Results: </strong>The AUCs for MACE at 30 days and 1 year were 0.645 and 0.650 (PORT), 0.633 and 0.661 (RCRI), and finally 0.489 and 0.557 (Gupta), respectively. The PORT model performed significantly better than the Gupta model at 1 year (<i>p</i>=0.039). When the sensitivity was set to 95%, PORT had a significantly higher specificity of 0.227 compared to RCRI's 0.071 (<i>p</i>=0.009) and Gupta's 0.08 (<i>p</i>=0.017). Our additional covariates increased the receiver operator curve from 0.664 to 0.703, but this did not reach statistical significance (<i>p</i>=0.278).</p><p><strong>Conclusions: </strong>Of the three calculators, PORT performed best when the sensitivity was set at a clinically relevant level. This is likely due to the unique variables the PORT model uses, which are specific to transplant patients.</p>","PeriodicalId":30584,"journal":{"name":"Surgery Research and Practice","volume":"2019 ","pages":"9080856"},"PeriodicalIF":0.0000,"publicationDate":"2019-03-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6446090/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgery Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2019/9080856","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Patients undergoing kidney transplantation have increased risk of adverse cardiovascular events due to histories of hypertension, end-stage renal disease, and dialysis. As such, they are especially in need of accurate preoperative risk assessment.
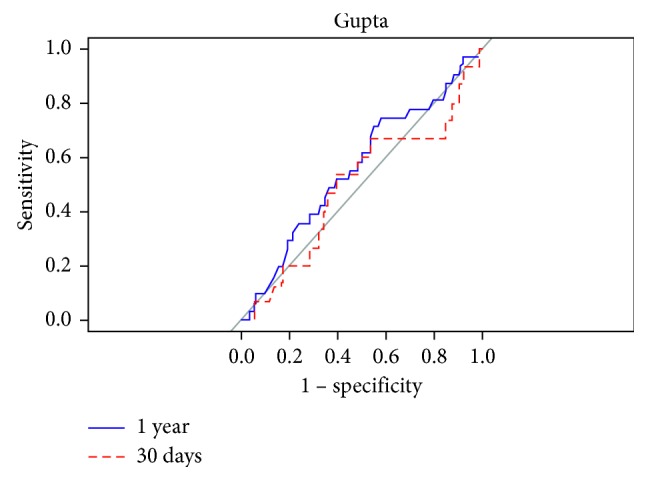
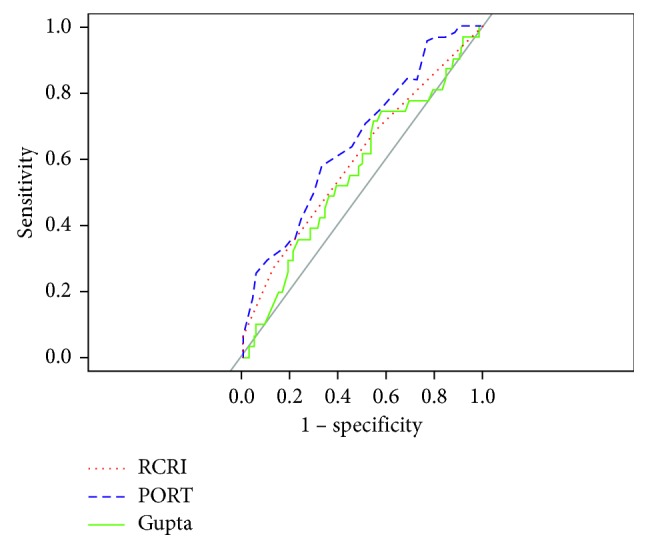
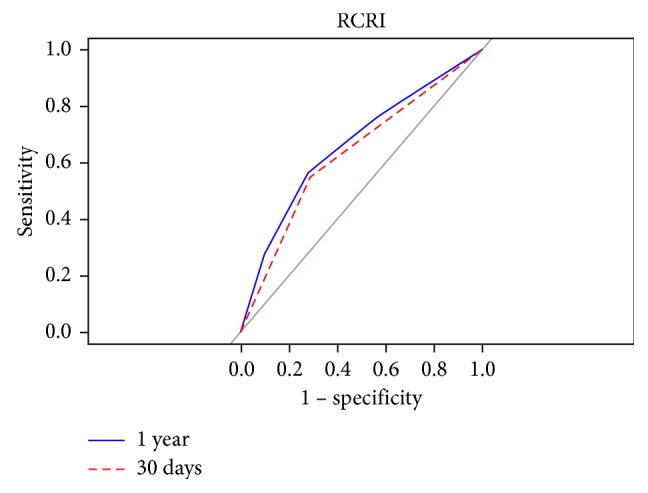
Methods: We compared three different risk assessment models for their ability to predict major adverse cardiac events at 30 days and 1 year after transplant. These were the PORT model, the RCRI model, and the Gupta model. We used a method based on generalized U-statistics to determine statistically significant improvements in the area under the receiver operator curve (AUC), based on a common major adverse cardiac event (MACE) definition. For the top-performing model, we added new covariates into multivariable logistic regression in an attempt to create further improvement in the AUC.
Results: The AUCs for MACE at 30 days and 1 year were 0.645 and 0.650 (PORT), 0.633 and 0.661 (RCRI), and finally 0.489 and 0.557 (Gupta), respectively. The PORT model performed significantly better than the Gupta model at 1 year (p=0.039). When the sensitivity was set to 95%, PORT had a significantly higher specificity of 0.227 compared to RCRI's 0.071 (p=0.009) and Gupta's 0.08 (p=0.017). Our additional covariates increased the receiver operator curve from 0.664 to 0.703, but this did not reach statistical significance (p=0.278).
Conclusions: Of the three calculators, PORT performed best when the sensitivity was set at a clinically relevant level. This is likely due to the unique variables the PORT model uses, which are specific to transplant patients.
期刊介绍:
Surgery Research and Practice is a peer-reviewed, Open Access journal that provides a forum for surgeons and the surgical research community. The journal publishes original research articles, review articles, and clinical studies focusing on clinical and laboratory research relevant to surgical practice and teaching, with an emphasis on findings directly affecting surgical management.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


