{"title":"False activation of the cardiac catheterization laboratory: The price to pay for shorter treatment delay.","authors":"George Degheim, Abeer Berry, Marcel Zughaib","doi":"10.1177/2048004019836365","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>In patients with acute ST elevation myocardial ischemia (STEMI), national efforts have focused on reducing door-to-balloon (D2B) times for primary percutaneous coronary intervention (PCI). This emphasis on time-to-treatment may increase the rate of inappropriate cardiac catheterization laboratory (CCL) activations and unnecessary healthcare utilization. To achieve lower D2B times, community hospitals and EMS systems have enabled emergency medical technicians (EMTs) and emergency department (ED) physicians to activate the CCLs without immediately consulting a cardiologist.</p><p><strong>Objective: </strong>The purpose of this study is to determine the rate and main causes of inappropriate activation of the CCL which will aid in finding solutions to reduce this occurrence.</p><p><strong>Method: </strong>This is a retrospective study, based on an electronic medical system review of all inappropriate CCL activation who presented to Providence Hospital and Medical Centers (PHMC) in Michigan, from January 2015 to July 2016.</p><p><strong>Results: </strong>The CCL was activated 375 times for suspected STEMI. The false STEMI activation was identified in 47 patients which represents 12.5% of total CCL activation. The vast majority of this false activation was due to non-diagnostic electrocardiogram (ECG) that did not meet the STEMI criteria.</p><p><strong>Conclusion: </strong>The subjective interpretation of the ECG by EMTs and ED physicians tend to show a wide variability, which may lead to higher-than-anticipated false activation rates of up to 36% in one study. Some studies had reported that up to 72% of inappropriate activations were caused by ECG misinterpretations. These false activations have ramifications that lead to both clinical and financial costs.</p>","PeriodicalId":30457,"journal":{"name":"JRSM Cardiovascular Disease","volume":"8 ","pages":"2048004019836365"},"PeriodicalIF":1.5000,"publicationDate":"2019-04-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/2048004019836365","citationCount":"8","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JRSM Cardiovascular Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2048004019836365","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 8
Abstract
Introduction: In patients with acute ST elevation myocardial ischemia (STEMI), national efforts have focused on reducing door-to-balloon (D2B) times for primary percutaneous coronary intervention (PCI). This emphasis on time-to-treatment may increase the rate of inappropriate cardiac catheterization laboratory (CCL) activations and unnecessary healthcare utilization. To achieve lower D2B times, community hospitals and EMS systems have enabled emergency medical technicians (EMTs) and emergency department (ED) physicians to activate the CCLs without immediately consulting a cardiologist.
Objective: The purpose of this study is to determine the rate and main causes of inappropriate activation of the CCL which will aid in finding solutions to reduce this occurrence.
Method: This is a retrospective study, based on an electronic medical system review of all inappropriate CCL activation who presented to Providence Hospital and Medical Centers (PHMC) in Michigan, from January 2015 to July 2016.
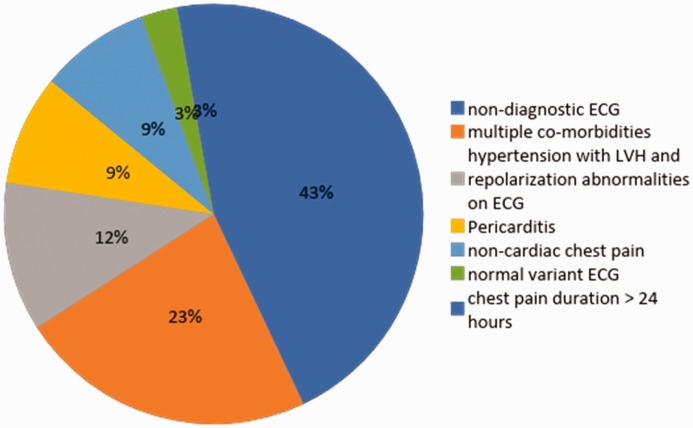
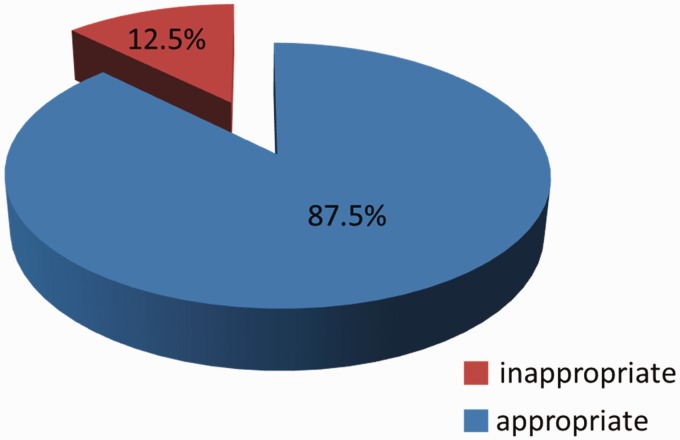
Results: The CCL was activated 375 times for suspected STEMI. The false STEMI activation was identified in 47 patients which represents 12.5% of total CCL activation. The vast majority of this false activation was due to non-diagnostic electrocardiogram (ECG) that did not meet the STEMI criteria.
Conclusion: The subjective interpretation of the ECG by EMTs and ED physicians tend to show a wide variability, which may lead to higher-than-anticipated false activation rates of up to 36% in one study. Some studies had reported that up to 72% of inappropriate activations were caused by ECG misinterpretations. These false activations have ramifications that lead to both clinical and financial costs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


