Praveen Ramakrishnan Geethakumari, Ashwin Sama, Jaime G Caro, Charles J Yeo, Srikanth Nagalla
{"title":"\"The Immune Conundrum\": Acquired Hemophilia A, Immune Thrombocytopenia, and Neutropenia in a Patient with Pancreatic Cancer.","authors":"Praveen Ramakrishnan Geethakumari, Ashwin Sama, Jaime G Caro, Charles J Yeo, Srikanth Nagalla","doi":"10.1089/crpc.2015.29011.prg","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Malignancy-associated bleeding can pose diagnostic dilemmas. We report a unique case of paraneoplastic acquired hemophilia A (AHA), immune thrombocytopenia (ITP), and immune neutropenia in a patient with pancreatic adenocarcinoma. <b>Case Presentation:</b> A 66-year-old male with newly diagnosed pancreatic cancer and normal preoperative hematological evaluation was taken to the operating room for pancreaticoduodenectomy. The operation was aborted due to empyema of the gall bladder, cholangitis, and local extent of disease. Postoperatively, the patient developed bleeding diatheses with mucocutaneous and intra-abdominal bleeding and a prolonged activated partial thromboplastin time. Evaluation revealed high-titer factor VIII inhibitor confirming AHA. Management with bypassing agents such as recombinant activated factor VII, factor VIII inhibitor bypassing activity, and immunosuppression with steroids, cyclophosphamide, and rituximab achieved remission in 2 months. ITP developed after achieving normal factor VIII levels, which was managed with intravenous immunoglobulin. Neutropenia was detected before initiation of chemotherapy and was managed with granulocyte-colony stimulating factor. <b>Conclusion:</b> These unique challenges posed by paraneoplastic hematological syndromes warrant the need for astute clinical judgment and multidisciplinary collaboration for effective management.</p>","PeriodicalId":92486,"journal":{"name":"Case reports in pancreatic cancer","volume":"2 1","pages":"14-18"},"PeriodicalIF":0.0000,"publicationDate":"2016-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1089/crpc.2015.29011.prg","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case reports in pancreatic cancer","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/crpc.2015.29011.prg","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
Abstract
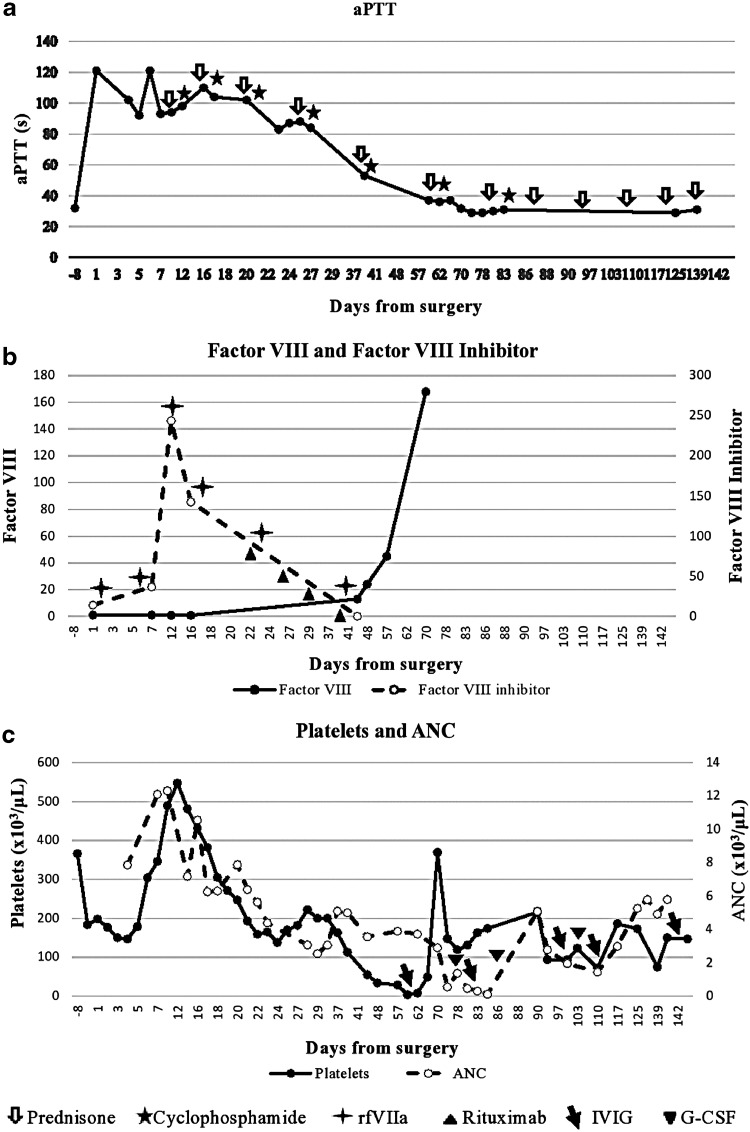
Background: Malignancy-associated bleeding can pose diagnostic dilemmas. We report a unique case of paraneoplastic acquired hemophilia A (AHA), immune thrombocytopenia (ITP), and immune neutropenia in a patient with pancreatic adenocarcinoma. Case Presentation: A 66-year-old male with newly diagnosed pancreatic cancer and normal preoperative hematological evaluation was taken to the operating room for pancreaticoduodenectomy. The operation was aborted due to empyema of the gall bladder, cholangitis, and local extent of disease. Postoperatively, the patient developed bleeding diatheses with mucocutaneous and intra-abdominal bleeding and a prolonged activated partial thromboplastin time. Evaluation revealed high-titer factor VIII inhibitor confirming AHA. Management with bypassing agents such as recombinant activated factor VII, factor VIII inhibitor bypassing activity, and immunosuppression with steroids, cyclophosphamide, and rituximab achieved remission in 2 months. ITP developed after achieving normal factor VIII levels, which was managed with intravenous immunoglobulin. Neutropenia was detected before initiation of chemotherapy and was managed with granulocyte-colony stimulating factor. Conclusion: These unique challenges posed by paraneoplastic hematological syndromes warrant the need for astute clinical judgment and multidisciplinary collaboration for effective management.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


