Katharina Ruf, Johannes Wirbelauer, Antje Beissert, Eric Frieauff
{"title":"Successful treatment of severe arterial hypotension and anuria in a preterm infant with renal tubular dysgenesis- a case report.","authors":"Katharina Ruf, Johannes Wirbelauer, Antje Beissert, Eric Frieauff","doi":"10.1186/s40748-018-0095-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Oligohydramnios sequence can be caused by renal tubular dysgenesis (RTD), a rare condition resulting in pulmonary and renal morbidity. Besides typical features of Potter-sequence, the infants present with severe arterial hypotension and anuria as main symptoms. Establishing an adequate arterial blood pressure and sufficient renal perfusion is crucial for the survival of these infants.</p><p><strong>Case presentation: </strong>We describe a male preterm infant of 34 + 0 weeks of gestation. Prenatally oligohydramnios of unknown cause was detected. After uneventful delivery and good adaptation the infant developed respiratory distress due to a spontaneous right-sided pneumothorax and required thoracocentesis and placement of a chest tube; he showed no major respiratory concerns thereafter and needed only minimal ventilatory support. Echocardiography revealed no abnormalities, especially no pulmonary hypertension. However, he suffered from severe arterial hypotension and anuria refractory to catecholamine therapy (dobutamine, epinephrine and noradrenaline). After 36 h of life, vasopressin therapy was initiated resulting in an almost immediate stabilization of arterial blood pressure and subsequent onset of diuresis. Therapy with vasopressin was necessary for three weeks to maintain adequate arterial blood pressure levels and diuresis. Sepsis and adrenal insufficiency were ruled out as inflammation markers, microbiological tests and cortisol level were normal. At two weeks of age, our patient developed electrolyte disturbances which were successfully treated with fludrocortisone. He did not need renal replacement therapy. Genetic analyses revealed a novel compound hyterozygous mutation of RTD. Now 17 months of age, the patient is in clinically stable condition with treatment of fludrocortisone and sodium bicarbonate. He suffers from stage 2 chronic kidney disease; blood pressure, motor and cognitive development are normal.</p><p><strong>Conclusions: </strong>RTD is a rare cause of oligohydramnios sequence. Next to pulmonary hypoplasia, severe arterial hypotension is responsible for poor survival. We present the only second surviving infant with RTD, who did not require renal replacement therapy during the neonatal period. It can be speculated whether the use of vasopressin prevents renal replacement therapy as vasopressin increases urinary output by improving renal blood flow.</p>","PeriodicalId":74120,"journal":{"name":"Maternal health, neonatology and perinatology","volume":"4 ","pages":"27"},"PeriodicalIF":0.0000,"publicationDate":"2018-12-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s40748-018-0095-z","citationCount":"8","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Maternal health, neonatology and perinatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40748-018-0095-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 8
Abstract
Background: Oligohydramnios sequence can be caused by renal tubular dysgenesis (RTD), a rare condition resulting in pulmonary and renal morbidity. Besides typical features of Potter-sequence, the infants present with severe arterial hypotension and anuria as main symptoms. Establishing an adequate arterial blood pressure and sufficient renal perfusion is crucial for the survival of these infants.
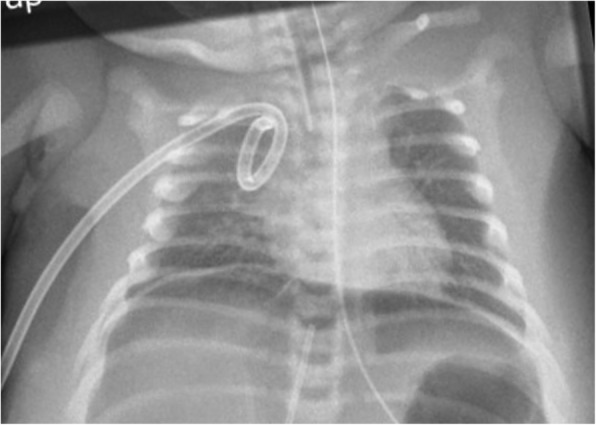
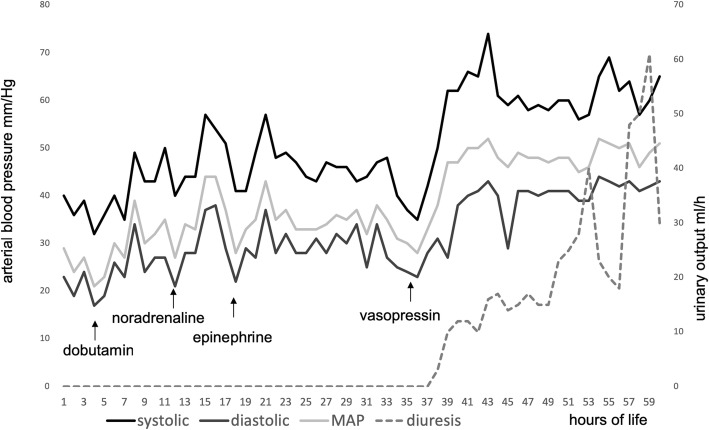
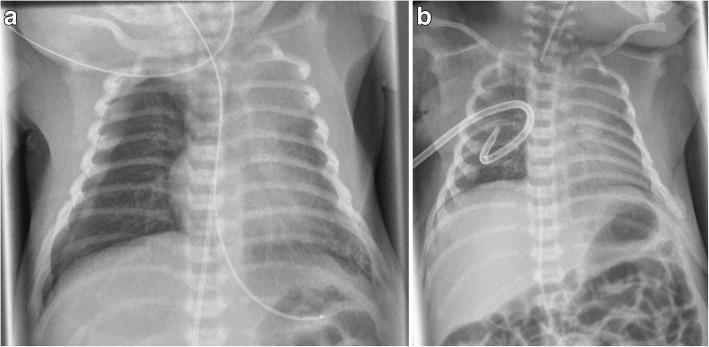
Case presentation: We describe a male preterm infant of 34 + 0 weeks of gestation. Prenatally oligohydramnios of unknown cause was detected. After uneventful delivery and good adaptation the infant developed respiratory distress due to a spontaneous right-sided pneumothorax and required thoracocentesis and placement of a chest tube; he showed no major respiratory concerns thereafter and needed only minimal ventilatory support. Echocardiography revealed no abnormalities, especially no pulmonary hypertension. However, he suffered from severe arterial hypotension and anuria refractory to catecholamine therapy (dobutamine, epinephrine and noradrenaline). After 36 h of life, vasopressin therapy was initiated resulting in an almost immediate stabilization of arterial blood pressure and subsequent onset of diuresis. Therapy with vasopressin was necessary for three weeks to maintain adequate arterial blood pressure levels and diuresis. Sepsis and adrenal insufficiency were ruled out as inflammation markers, microbiological tests and cortisol level were normal. At two weeks of age, our patient developed electrolyte disturbances which were successfully treated with fludrocortisone. He did not need renal replacement therapy. Genetic analyses revealed a novel compound hyterozygous mutation of RTD. Now 17 months of age, the patient is in clinically stable condition with treatment of fludrocortisone and sodium bicarbonate. He suffers from stage 2 chronic kidney disease; blood pressure, motor and cognitive development are normal.
Conclusions: RTD is a rare cause of oligohydramnios sequence. Next to pulmonary hypoplasia, severe arterial hypotension is responsible for poor survival. We present the only second surviving infant with RTD, who did not require renal replacement therapy during the neonatal period. It can be speculated whether the use of vasopressin prevents renal replacement therapy as vasopressin increases urinary output by improving renal blood flow.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


