{"title":"Acute pancreatitis after major spine surgery: a case report and literature review.","authors":"Daniela Ghisi, Alessandro Ricci, Sandra Giannone, Tiziana Greggi, Stefano Bonarelli","doi":"10.1186/s13013-018-0170-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute pancreatitis has been described as potential complication of both abdominal and non-abdominal surgeries. The pathogenetic mechanism underlying acute pancreatitis in spine surgery may include intraoperative hemodynamic instability causing prolonged splanchnic hypoperfusion, as well as mechanical compression of the pancreas due to scoliosis correction, with a higher risk in cases of more extended fusions, especially in young adults with lower body mass index (BMI).</p><p><strong>Case presentation: </strong>We report here a case of postoperative acute pancreatitis with benign evolution in a young female patient after the first and second surgery of a two-stage correction of right thoracic idiopathic scoliosis.In December 2017, the patient underwent first-stage T4-L3 posterior arthrodesis with T7-T12 osteotomies and temporary magnetic bar. Intraoperative blood loss required massive transfusion. In the immediate postoperative period, the patient started reporting nausea/vomiting, abdominal pain at pressure, moderate meteorism, abdominal distension, hypoactive bowel sounds, and fever. Laboratory tests indicated a progressive increase in aspartate aminotransferase, alanine aminotransferase, serum amylase, lipase, phospho-creatine kinase, and reactive C-protein. A CT scan showed free abundant abdominal fluid in the hepatic, renal, pancreatic, and pelvic regions. After the diagnosis, a hypolipidic diet was initiated, and good hydration per os was maintained. After gastroenterologic consultation, somatostatin, rifaximin, and ursodehoxycholic acid were initiated and maintained for 8 days. In the following days, laboratory tests showed a slow but consistent decrease in liver and pancreatic enzymes until normalization. In January 2018, the patient underwent second-stage surgery with removal of magnetic bar, definitive posterior fusion, and instrumentation T4-L3. Laboratory tests showed a second, even more significant, increase in the amylase and lipase level and a moderate increase in the reactive C-protein. Therapy was maintained until complete normalization of amylase and lipase levels.</p><p><strong>Conclusions: </strong>Early recognition of symptoms plays a key role in preventing severe morbidity after scoliosis surgery. When symptoms suggest abdominal complication, pancreatic and liver enzymes are to be evaluated for posing prompt diagnosis. Gastroenterologic consultation and eventual imaging are further steps in differential diagnosis and treatment of this rare complication.</p>","PeriodicalId":21573,"journal":{"name":"Scoliosis and Spinal Disorders","volume":"13 ","pages":"24"},"PeriodicalIF":0.0000,"publicationDate":"2018-11-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s13013-018-0170-2","citationCount":"5","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scoliosis and Spinal Disorders","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13013-018-0170-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 5
Abstract
Background: Acute pancreatitis has been described as potential complication of both abdominal and non-abdominal surgeries. The pathogenetic mechanism underlying acute pancreatitis in spine surgery may include intraoperative hemodynamic instability causing prolonged splanchnic hypoperfusion, as well as mechanical compression of the pancreas due to scoliosis correction, with a higher risk in cases of more extended fusions, especially in young adults with lower body mass index (BMI).
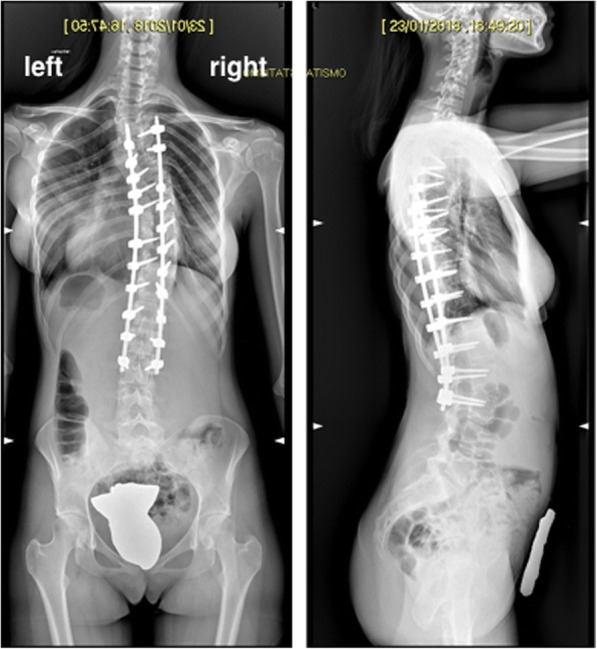
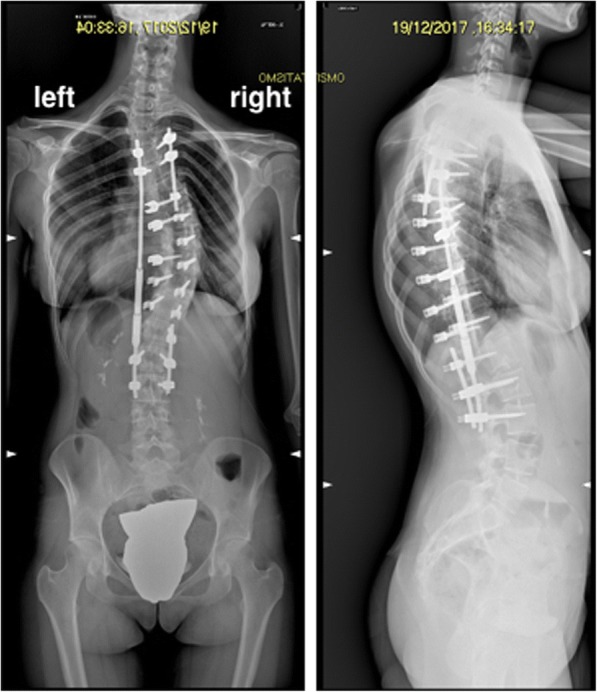
Case presentation: We report here a case of postoperative acute pancreatitis with benign evolution in a young female patient after the first and second surgery of a two-stage correction of right thoracic idiopathic scoliosis.In December 2017, the patient underwent first-stage T4-L3 posterior arthrodesis with T7-T12 osteotomies and temporary magnetic bar. Intraoperative blood loss required massive transfusion. In the immediate postoperative period, the patient started reporting nausea/vomiting, abdominal pain at pressure, moderate meteorism, abdominal distension, hypoactive bowel sounds, and fever. Laboratory tests indicated a progressive increase in aspartate aminotransferase, alanine aminotransferase, serum amylase, lipase, phospho-creatine kinase, and reactive C-protein. A CT scan showed free abundant abdominal fluid in the hepatic, renal, pancreatic, and pelvic regions. After the diagnosis, a hypolipidic diet was initiated, and good hydration per os was maintained. After gastroenterologic consultation, somatostatin, rifaximin, and ursodehoxycholic acid were initiated and maintained for 8 days. In the following days, laboratory tests showed a slow but consistent decrease in liver and pancreatic enzymes until normalization. In January 2018, the patient underwent second-stage surgery with removal of magnetic bar, definitive posterior fusion, and instrumentation T4-L3. Laboratory tests showed a second, even more significant, increase in the amylase and lipase level and a moderate increase in the reactive C-protein. Therapy was maintained until complete normalization of amylase and lipase levels.
Conclusions: Early recognition of symptoms plays a key role in preventing severe morbidity after scoliosis surgery. When symptoms suggest abdominal complication, pancreatic and liver enzymes are to be evaluated for posing prompt diagnosis. Gastroenterologic consultation and eventual imaging are further steps in differential diagnosis and treatment of this rare complication.
期刊介绍:
Cessation.Scoliosis and Spinal Disorders is an open access, multidisciplinary journal that encompasses all aspects of research on prevention, diagnosis, treatment, outcomes and cost-analyses of conservative and surgical management of all spinal deformities and disorders. Both clinical and basic science reports form the cornerstone of the journal in its endeavour to provide original, primary studies as well as narrative/systematic reviews and meta-analyses to the academic community and beyond. Scoliosis and Spinal Disorders aims to provide an integrated and balanced view of cutting-edge spine research to further enhance effective collaboration among clinical spine specialists and scientists, and to ultimately improve patient outcomes based on an evidence-based spine care approach.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


