Massive Subcutaneous Emphysema, Pneumoperitoneum, Pneumoretroperitoneum, and Pneumoscrotum following Endoscopic Retrograde Cholangiopancreatography in a Living Liver Donor.
{"title":"Massive Subcutaneous Emphysema, Pneumoperitoneum, Pneumoretroperitoneum, and Pneumoscrotum following Endoscopic Retrograde Cholangiopancreatography in a Living Liver Donor.","authors":"S Akbulut, B Isik, Y Karipkiz, S Yilmaz","doi":"","DOIUrl":null,"url":null,"abstract":"<p><p>Despite having many advantages, living donor liver transplantation has not been adopted by western countries due to risk of nearly life-threatening complications after living donor hepatectomy (LDH). Herein, we aimed at presenting the management of a 19-year-old patient who suffered life-threatening complications after right lobe LDH. A multiple detector computed tomography (MDCT) revealed a bilioma at the cut surface of the remnant liver, for which a transhepatic drainage catheter was placed. Endoscopic retrograde cholangiopancreatography (ERCP) performed to decompress biliary tract, but the biliary tract could not be cannulized due to post-precut bleeding. On the next day, extensive crepitation was detected and MDCT showed subcutaneous emphysema, pneumoperitoneum, pneumoretroperitoneum, and pneumoscrotum (ERCP-related duodenal perforation?). However, the patient showed significant deterioration of physical examination findings, fever, and infectious parameters, and therefore was taken to the operating room. Kocher maneuver revealed no apparent duodenal perforation. Then, a 2-mm bile duct was found open at the caudate lobe, through which bile leaked. Then, common bile duct exploration and T-tube placement were performed, followed by suture closure of the bile orifice at the caudate lobe. Massive air previously identified completely disappeared one week after the operation.</p>","PeriodicalId":14242,"journal":{"name":"International Journal of Organ Transplantation Medicine","volume":"9 3","pages":"132-135"},"PeriodicalIF":0.2000,"publicationDate":"2018-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6252177/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Organ Transplantation Medicine","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/8/1 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
引用次数: 0
Abstract
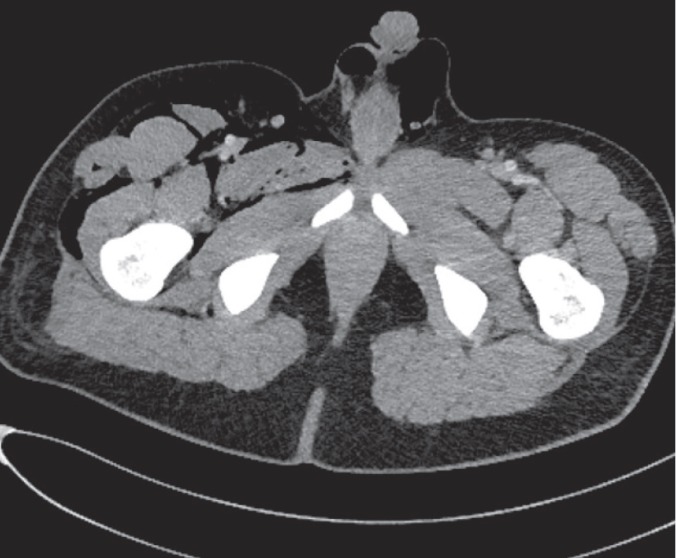
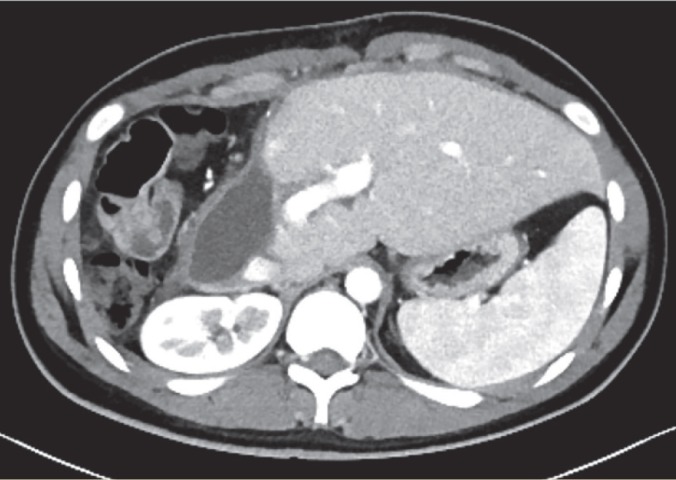
Despite having many advantages, living donor liver transplantation has not been adopted by western countries due to risk of nearly life-threatening complications after living donor hepatectomy (LDH). Herein, we aimed at presenting the management of a 19-year-old patient who suffered life-threatening complications after right lobe LDH. A multiple detector computed tomography (MDCT) revealed a bilioma at the cut surface of the remnant liver, for which a transhepatic drainage catheter was placed. Endoscopic retrograde cholangiopancreatography (ERCP) performed to decompress biliary tract, but the biliary tract could not be cannulized due to post-precut bleeding. On the next day, extensive crepitation was detected and MDCT showed subcutaneous emphysema, pneumoperitoneum, pneumoretroperitoneum, and pneumoscrotum (ERCP-related duodenal perforation?). However, the patient showed significant deterioration of physical examination findings, fever, and infectious parameters, and therefore was taken to the operating room. Kocher maneuver revealed no apparent duodenal perforation. Then, a 2-mm bile duct was found open at the caudate lobe, through which bile leaked. Then, common bile duct exploration and T-tube placement were performed, followed by suture closure of the bile orifice at the caudate lobe. Massive air previously identified completely disappeared one week after the operation.
期刊介绍:
The International Journal of Organ Transplantation Medicine (IJOTM) is a quarterly peer-reviewed English-language journal that publishes high-quality basic sciences and clinical research on transplantation. The scope of the journal includes organ and tissue donation, procurement and preservation; surgical techniques, innovations, and novelties in all aspects of transplantation; genomics and immunobiology; immunosuppressive drugs and pharmacology relevant to transplantation; graft survival and prevention of graft dysfunction and failure; clinical trials and population analyses in the field of transplantation; transplant complications; cell and tissue transplantation; infection; post-transplant malignancies; sociological and ethical issues and xenotransplantation.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


