{"title":"An X-Linked Hyper-IgM Patient Followed Successfully for 23 Years without Hematopoietic Stem Cell Transplantation.","authors":"Necil Kutukculer, Neslihan Edeer Karaca, Guzide Aksu, Ayca Aykut, Erhan Pariltay, Ozgur Cogulu","doi":"10.1155/2018/6897935","DOIUrl":null,"url":null,"abstract":"<p><p>When caring for patients with life-limiting diseases, improving survival and optimizing quality of life are the primary goals. For patients with X-linked hyper-IgM syndrome (XHIGM), the treatment modality has to be decided for a particular patient regarding hematopoietic stem cell transplantation or intravenous immunoglobulin replacement therapy with <i>P. jiroveci</i> prophylaxis. A seven-year-old male patient was admitted with recurrent upper and lower respiratory tract infections and recurrent otitis media. His initial immunologic evaluation revealed low IgG and normal IgA and IgM levels with normal lymphocyte phenotyping and inadequate specific antibody responses. He was diagnosed as common variable immunodeficiency and began to receive intravenous immunoglobulin (IVIG) (0.5 gm/kg) with four-week intervals. During follow-up for 23 years under IVIG therapy, he was extremely well and never had severe infections. In 2017, targeted next generation sequencing was performed in order to understand his molecular pathology. A previously described hemizygous c.31C>T(p.Arg11Ter) mutation was found in <i>CD40LG</i> gene. The mother was heterozygous carrier for this mutation and his sister did not have any mutation. Flow cytometric analysis for <i>CD40LG</i> expression on activated T cells showed highly decreased, but not absent, <i>CD40LG</i> expression. In conclusion, diagnostic delay is a clinical problem for patients with <i>CD40LG</i> deficiency, because of low or normal IgM levels, showing that all the hypogammaglobulinemic patients, not only with high serum IgM levels, but also with normal to low IgM levels, have to be examined for <i>CD40LG</i> expression on activated T lymphocytes. Secondly, type of <i>CD40LG</i> mutations leads to enormous interpatient variations regarding serum IgM levels, CD40LG levels on activated T cells, age at diagnosis, severity of clinical findings, and follow-up therapies with or without hematopoietic stem cell therapy.</p>","PeriodicalId":42865,"journal":{"name":"Case Reports in Immunology","volume":"2018 ","pages":"6897935"},"PeriodicalIF":1.5000,"publicationDate":"2018-10-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2018/6897935","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Immunology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2018/6897935","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 4
Abstract
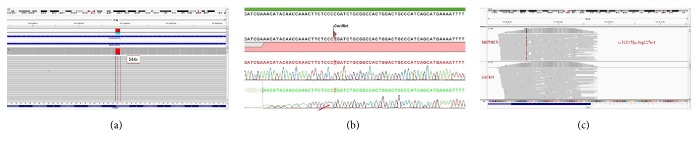
When caring for patients with life-limiting diseases, improving survival and optimizing quality of life are the primary goals. For patients with X-linked hyper-IgM syndrome (XHIGM), the treatment modality has to be decided for a particular patient regarding hematopoietic stem cell transplantation or intravenous immunoglobulin replacement therapy with P. jiroveci prophylaxis. A seven-year-old male patient was admitted with recurrent upper and lower respiratory tract infections and recurrent otitis media. His initial immunologic evaluation revealed low IgG and normal IgA and IgM levels with normal lymphocyte phenotyping and inadequate specific antibody responses. He was diagnosed as common variable immunodeficiency and began to receive intravenous immunoglobulin (IVIG) (0.5 gm/kg) with four-week intervals. During follow-up for 23 years under IVIG therapy, he was extremely well and never had severe infections. In 2017, targeted next generation sequencing was performed in order to understand his molecular pathology. A previously described hemizygous c.31C>T(p.Arg11Ter) mutation was found in CD40LG gene. The mother was heterozygous carrier for this mutation and his sister did not have any mutation. Flow cytometric analysis for CD40LG expression on activated T cells showed highly decreased, but not absent, CD40LG expression. In conclusion, diagnostic delay is a clinical problem for patients with CD40LG deficiency, because of low or normal IgM levels, showing that all the hypogammaglobulinemic patients, not only with high serum IgM levels, but also with normal to low IgM levels, have to be examined for CD40LG expression on activated T lymphocytes. Secondly, type of CD40LG mutations leads to enormous interpatient variations regarding serum IgM levels, CD40LG levels on activated T cells, age at diagnosis, severity of clinical findings, and follow-up therapies with or without hematopoietic stem cell therapy.
期刊介绍:
Case Reports in Immunology is a peer-reviewed, Open Access journal that publishes case reports and case series related to allergies, immunodeficiencies, autoimmune diseases, immune disorders, cancer immunology and transplantation immunology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


