Overlap Anastomosis for Digestive Reconstruction during Laparoscopic Distal Gastrectomy with Intensive Regional Lymph Node Dissection: Physiological Impact of Preserving the Mesenteric Autonomic Nerves in the Lifted Jejunal Limb.
Taku Kitano, Daiki Yasukawa, Yuki Aisu, Tomohide Hori
{"title":"Overlap Anastomosis for Digestive Reconstruction during Laparoscopic Distal Gastrectomy with Intensive Regional Lymph Node Dissection: Physiological Impact of Preserving the Mesenteric Autonomic Nerves in the Lifted Jejunal Limb.","authors":"Taku Kitano, Daiki Yasukawa, Yuki Aisu, Tomohide Hori","doi":"10.1155/2018/4938341","DOIUrl":null,"url":null,"abstract":"<p><p>Laparoscopic gastrectomy is a treatment for gastric cancer, and isoperistaltic side-to-side reconstruction is called \"overlap anastomosis.\" The physiological advantages of preserving the autonomic nerves in the jejunal limb for digestive reconstruction are well known. Here, we focused on overlap anastomosis with autonomic nerve-preserved mesojejunum of the lifted jejunal limb for laparoscopic distal gastrectomy with intentional lymph node dissection. Our surgical techniques and technical pitfalls were described in detail. The jejunum was partially sacrificed to preserve the autonomic nerves in the lifted jejunal limb. The length of the staple line was 35 - 40 mm. The endostapler entry was carefully closed to avoid even subtle stenosis. Twelve patients were retrospectively evaluated with a follow-up of 5.0 ± 0.6 years. Histological findings according to the Japanese classification were stage IA or IB. Dietary intake and postoperative ambulation occurred at 3.3 ± 1.0 and 1.3 ± 0.5 days after surgery, respectively. Postoperative complications according to Clavien-Dindo classification were one each of grade I and grade II. Postoperative hospital stay was 6.7 ± 1.6 days. Five patients were medication-free at final follow-up, with no recurrence in any patient. Overlap anastomosis with autonomic nerve-preserved jejunal limb was safe and feasible for laparoscopic distal gastrectomy with lymph node dissection.</p>","PeriodicalId":30584,"journal":{"name":"Surgery Research and Practice","volume":"2018 ","pages":"4938341"},"PeriodicalIF":0.0000,"publicationDate":"2018-09-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2018/4938341","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgery Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2018/4938341","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
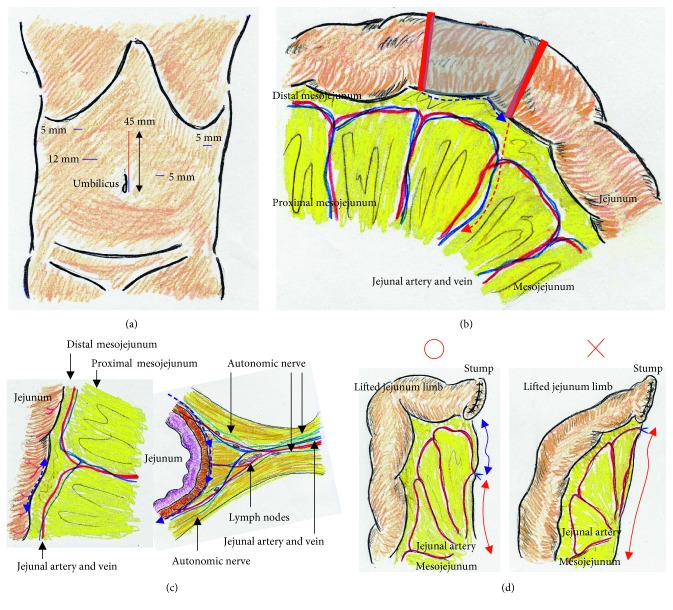
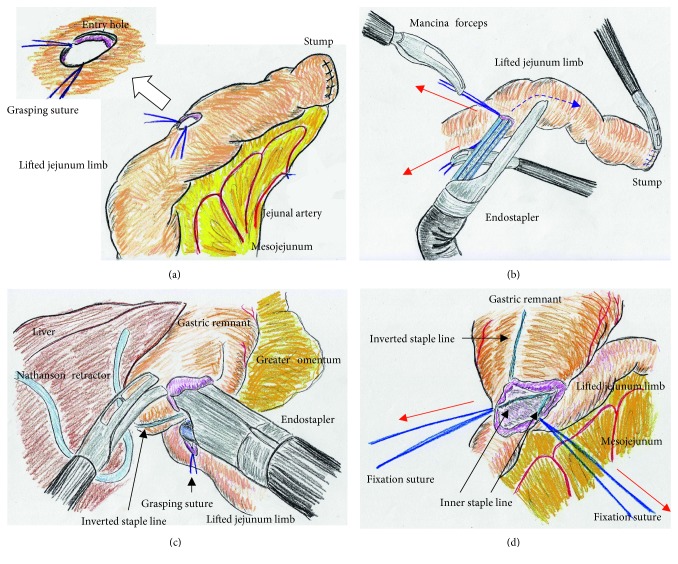
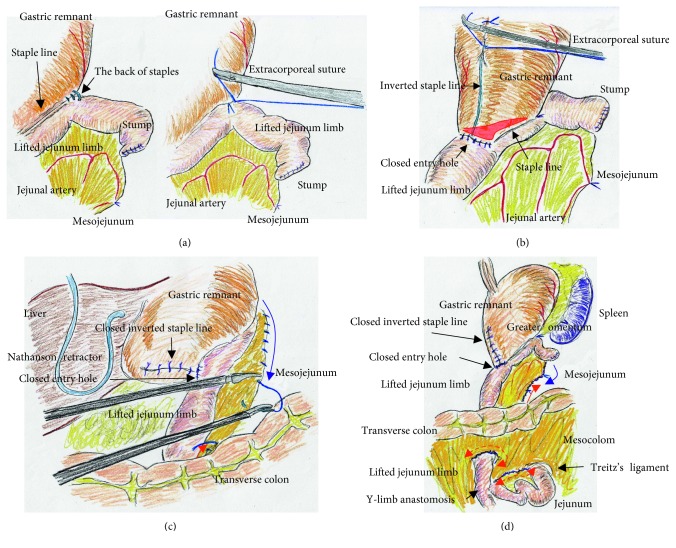
Laparoscopic gastrectomy is a treatment for gastric cancer, and isoperistaltic side-to-side reconstruction is called "overlap anastomosis." The physiological advantages of preserving the autonomic nerves in the jejunal limb for digestive reconstruction are well known. Here, we focused on overlap anastomosis with autonomic nerve-preserved mesojejunum of the lifted jejunal limb for laparoscopic distal gastrectomy with intentional lymph node dissection. Our surgical techniques and technical pitfalls were described in detail. The jejunum was partially sacrificed to preserve the autonomic nerves in the lifted jejunal limb. The length of the staple line was 35 - 40 mm. The endostapler entry was carefully closed to avoid even subtle stenosis. Twelve patients were retrospectively evaluated with a follow-up of 5.0 ± 0.6 years. Histological findings according to the Japanese classification were stage IA or IB. Dietary intake and postoperative ambulation occurred at 3.3 ± 1.0 and 1.3 ± 0.5 days after surgery, respectively. Postoperative complications according to Clavien-Dindo classification were one each of grade I and grade II. Postoperative hospital stay was 6.7 ± 1.6 days. Five patients were medication-free at final follow-up, with no recurrence in any patient. Overlap anastomosis with autonomic nerve-preserved jejunal limb was safe and feasible for laparoscopic distal gastrectomy with lymph node dissection.
期刊介绍:
Surgery Research and Practice is a peer-reviewed, Open Access journal that provides a forum for surgeons and the surgical research community. The journal publishes original research articles, review articles, and clinical studies focusing on clinical and laboratory research relevant to surgical practice and teaching, with an emphasis on findings directly affecting surgical management.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


