Franck Le Navéaux, A Noelle Larson, Hubert Labelle, Carl-Eric Aubin
{"title":"Significant variability in surgeons' preferred correction maneuvers and instrumentation strategies when planning adolescent idiopathic scoliosis surgery.","authors":"Franck Le Navéaux, A Noelle Larson, Hubert Labelle, Carl-Eric Aubin","doi":"10.1186/s13013-018-0169-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Increased implant number is thought to provide better control on the scoliotic spine, but there is limited scientific evidence of improved deformity correction and surgical outcomes with high-density constructs. The objective is to assess key anchor points used by experienced spinal deformity surgeons and to evaluate the effect of implant density pattern on correction techniques.</p><p><strong>Methods: </strong>Seventeen experienced spine surgeons reviewed five Lenke 1 adolescent idiopathic scoliosis cases and provided their preferred posterior correction technique (implant pattern, correction maneuvers, and implants used for their execution) and an alternative technique with the minimal implant density they felt would be acceptable (170 surgical plans total). Additionally, for each case, they selected acceptable screw patterns for surgery from seven published implant configurations. Variability in the surgeons' plans was assessed, including instrumentation and correction strategies.</p><p><strong>Results: </strong>The preferred correction plan involved an average of 1.65 implants/vertebra, with 88% of the available anchor points at the apex ± 1 vertebra used for the execution of correction maneuvers and only 43% of possible anchor points used proximal and distal to the apical area. The minimal density that surgeons found acceptable was 1.24 implants/vertebra. The minimal density plan involved more in situ rod contouring (53 vs. 41%), fewer vertebral derotation maneuvers (82 vs. 96%), and fewer implants used for compression/distraction maneuvers (1.18 and 1.42 respectively) (<i>p</i> < 0.05). Implant placement at alternate levels or dropout of convex implants above and below the apical area was most frequently considered acceptable (> 70% agreement).</p><p><strong>Conclusions: </strong>Implant position and number affect surgeons correction maneuvers selection. For low implant density constructs, dropout in the convexity and particularly in the periapical region is accepted by surgeons, with minor influence on planned correction maneuvers. Thus, preoperative implant planning must take into account which anchor points are needed for desired correction maneuvers.</p>","PeriodicalId":21573,"journal":{"name":"Scoliosis and Spinal Disorders","volume":"13 ","pages":"21"},"PeriodicalIF":0.0000,"publicationDate":"2018-10-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6174067/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scoliosis and Spinal Disorders","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13013-018-0169-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Increased implant number is thought to provide better control on the scoliotic spine, but there is limited scientific evidence of improved deformity correction and surgical outcomes with high-density constructs. The objective is to assess key anchor points used by experienced spinal deformity surgeons and to evaluate the effect of implant density pattern on correction techniques.
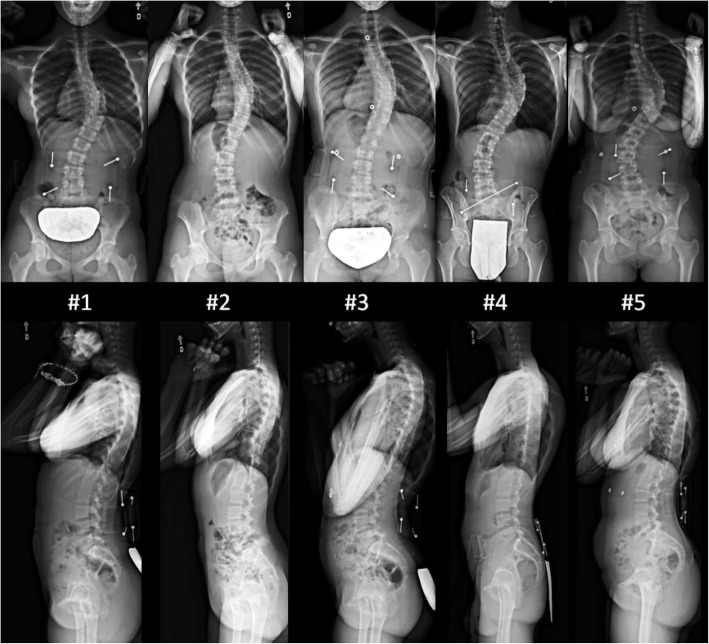
Methods: Seventeen experienced spine surgeons reviewed five Lenke 1 adolescent idiopathic scoliosis cases and provided their preferred posterior correction technique (implant pattern, correction maneuvers, and implants used for their execution) and an alternative technique with the minimal implant density they felt would be acceptable (170 surgical plans total). Additionally, for each case, they selected acceptable screw patterns for surgery from seven published implant configurations. Variability in the surgeons' plans was assessed, including instrumentation and correction strategies.
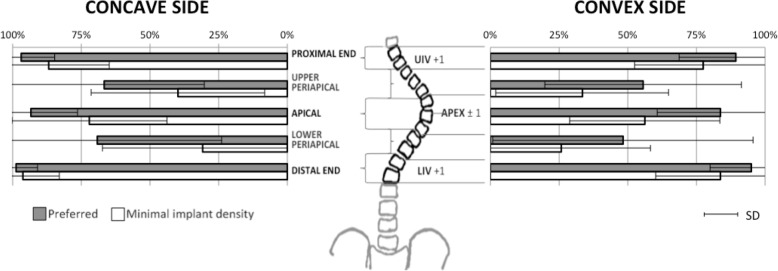
Results: The preferred correction plan involved an average of 1.65 implants/vertebra, with 88% of the available anchor points at the apex ± 1 vertebra used for the execution of correction maneuvers and only 43% of possible anchor points used proximal and distal to the apical area. The minimal density that surgeons found acceptable was 1.24 implants/vertebra. The minimal density plan involved more in situ rod contouring (53 vs. 41%), fewer vertebral derotation maneuvers (82 vs. 96%), and fewer implants used for compression/distraction maneuvers (1.18 and 1.42 respectively) (p < 0.05). Implant placement at alternate levels or dropout of convex implants above and below the apical area was most frequently considered acceptable (> 70% agreement).
Conclusions: Implant position and number affect surgeons correction maneuvers selection. For low implant density constructs, dropout in the convexity and particularly in the periapical region is accepted by surgeons, with minor influence on planned correction maneuvers. Thus, preoperative implant planning must take into account which anchor points are needed for desired correction maneuvers.
期刊介绍:
Cessation.Scoliosis and Spinal Disorders is an open access, multidisciplinary journal that encompasses all aspects of research on prevention, diagnosis, treatment, outcomes and cost-analyses of conservative and surgical management of all spinal deformities and disorders. Both clinical and basic science reports form the cornerstone of the journal in its endeavour to provide original, primary studies as well as narrative/systematic reviews and meta-analyses to the academic community and beyond. Scoliosis and Spinal Disorders aims to provide an integrated and balanced view of cutting-edge spine research to further enhance effective collaboration among clinical spine specialists and scientists, and to ultimately improve patient outcomes based on an evidence-based spine care approach.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


