Combined lung and brain ultrasonography for an individualized "brain-protective ventilation strategy" in neurocritical care patients with challenging ventilation needs.
IF 3.6 Q1 RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING
Francesco Corradi, Chiara Robba, Guido Tavazzi, Gabriele Via
{"title":"Combined lung and brain ultrasonography for an individualized \"brain-protective ventilation strategy\" in neurocritical care patients with challenging ventilation needs.","authors":"Francesco Corradi, Chiara Robba, Guido Tavazzi, Gabriele Via","doi":"10.1186/s13089-018-0105-4","DOIUrl":null,"url":null,"abstract":"<p><p>When intracranial hypertension and severe lung damage coexist in the same clinical scenario, their management poses a difficult challenge, especially as concerns mechanical ventilation management. The needs of combined lung and brain protection from secondary damage may conflict, as ventilation strategies commonly used in patients with ARDS are potentially associated with an increased risk of intracranial hypertension. In particular, the use of positive end-expiratory pressure, recruitment maneuvers, prone positioning, and protective lung ventilation can have undesirable effects on cerebral physiology: they may positively or negatively affect intracranial pressure, based on the final repercussions on PaO<sub>2</sub> and cerebral perfusion pressure (through changes in cardiac output, mean arterial pressure, venous return, PaO<sub>2</sub> and PaCO<sub>2</sub>), also according to the baseline conditions of cerebral autoregulation. Lung ultrasound (LUS) and brain ultrasound (BUS, as a combination of optic nerve sheath diameter assessment and cerebrovascular Doppler ultrasound) have independently proven their potential in respectively monitoring lung aeration and brain physiology at the bedside. In this narrative review, we describe how the combined use of LUS and BUS on neurocritical patients with demanding mechanical ventilation needs can contribute to ventilation management, with the aim of a tailored \"brain-protective ventilation strategy.\"</p>","PeriodicalId":46598,"journal":{"name":"Critical Ultrasound Journal","volume":"10 1","pages":"24"},"PeriodicalIF":3.6000,"publicationDate":"2018-09-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s13089-018-0105-4","citationCount":"14","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Ultrasound Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-018-0105-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 14
Abstract
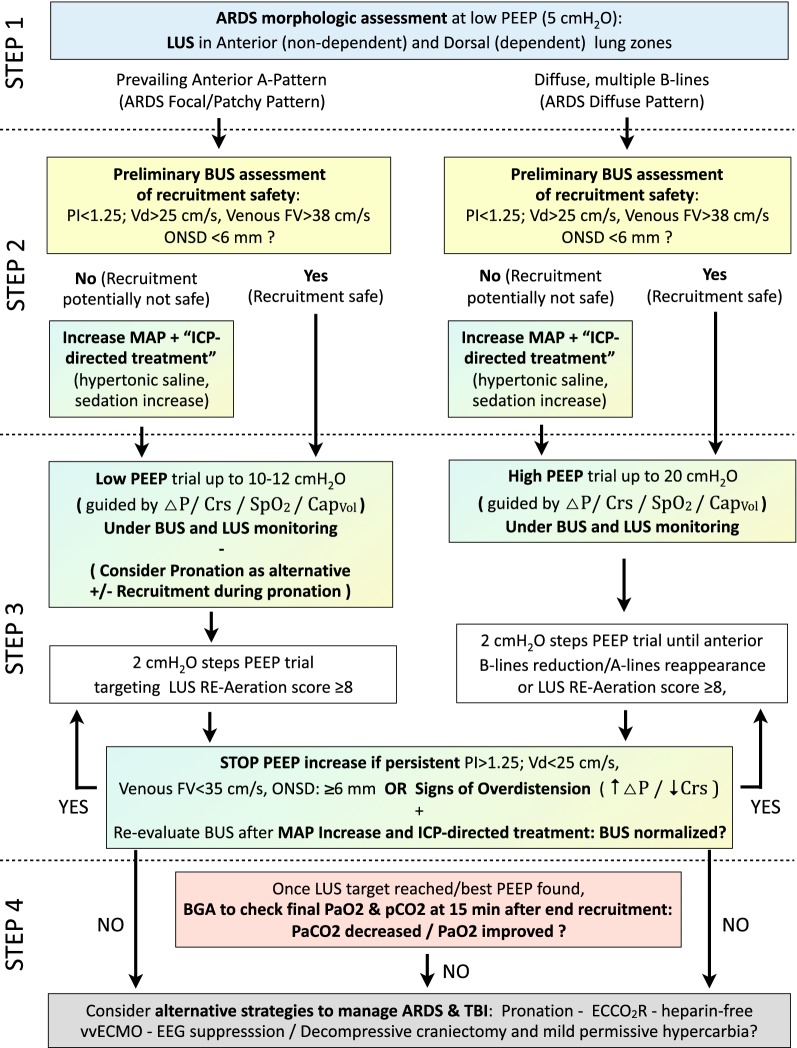
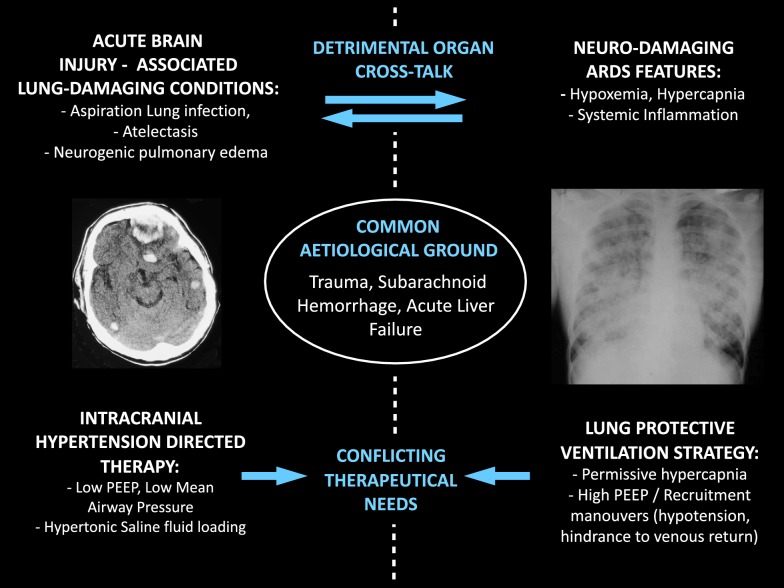
When intracranial hypertension and severe lung damage coexist in the same clinical scenario, their management poses a difficult challenge, especially as concerns mechanical ventilation management. The needs of combined lung and brain protection from secondary damage may conflict, as ventilation strategies commonly used in patients with ARDS are potentially associated with an increased risk of intracranial hypertension. In particular, the use of positive end-expiratory pressure, recruitment maneuvers, prone positioning, and protective lung ventilation can have undesirable effects on cerebral physiology: they may positively or negatively affect intracranial pressure, based on the final repercussions on PaO2 and cerebral perfusion pressure (through changes in cardiac output, mean arterial pressure, venous return, PaO2 and PaCO2), also according to the baseline conditions of cerebral autoregulation. Lung ultrasound (LUS) and brain ultrasound (BUS, as a combination of optic nerve sheath diameter assessment and cerebrovascular Doppler ultrasound) have independently proven their potential in respectively monitoring lung aeration and brain physiology at the bedside. In this narrative review, we describe how the combined use of LUS and BUS on neurocritical patients with demanding mechanical ventilation needs can contribute to ventilation management, with the aim of a tailored "brain-protective ventilation strategy."


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


