Luisa María Ricaurte, Oscar Arrieta, Zyanya Lucia Zatarain-Barrón, Andrés F Cardona
{"title":"Comprehensive review of fetal adenocarcinoma of the lung.","authors":"Luisa María Ricaurte, Oscar Arrieta, Zyanya Lucia Zatarain-Barrón, Andrés F Cardona","doi":"10.2147/LCTT.S137410","DOIUrl":null,"url":null,"abstract":"<p><p>Fetal adenocarcinoma of the lung (FLAC) is a rare tumor. It accounts for ~0.1%-0.5% of all pulmonary neoplasms. Due to its rarity, much of the world literature regarding FLAC comes from case reports and case series. FLAC is an adenocarcinoma resembling developing fetal lung in its pseudoglandular stage (8-16 weeks of gestation). It is distinguishable from pulmonary blastoma (PB) because it lacks the mesenchymal component which is a hallmark finding in PB. Due to differences in histopathology and clinical course, FLAC has been further categorized into low-grade (L-FLAC) and high-grade (H-FLAC) forms. L-FLAC displays low nuclear atypia and prominent morule formation and has a pure pattern. H-FLAC typically presents with at least 50% fetal morphology, and is often associated with other conventional types of lung adenocarcinoma. FLAC expresses neuroendocrine markers and thyroid transcription factor 1 in most cases. L-FLAC has an aberrant nuclear/cytoplasmic expression of β-catenin and presents mutations in this gene. H-FLAC overexpresses p53. These tumors have a very low frequency of mutations in <i>KRAS</i> and <i>EGFR</i>; it is thought that they are different from a molecular point of view to conventional lung adenocarcinomas. Approximately 25%-40% of patients are asymptomatic at presentation; most of them are incidental findings on chest radiographs. H-FLAC is more common in elderly male patients, with a heavy smoking history. L-FLAC tends to occur in young females. Patients with L-FLAC are usually diagnosed with stage I-II disease, while patients with H-FLAC usually present with a more advanced-stage disease. Poor prognostic factors for FLAC are thoracic lymphadenopathy, metastases at diagnosis, and tumor recurrence; however, the 10-year survival for FLAC is estimated at 75%.</p>","PeriodicalId":18066,"journal":{"name":"Lung Cancer: Targets and Therapy","volume":null,"pages":null},"PeriodicalIF":5.1000,"publicationDate":"2018-08-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.2147/LCTT.S137410","citationCount":"18","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Lung Cancer: Targets and Therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/LCTT.S137410","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 18
Abstract
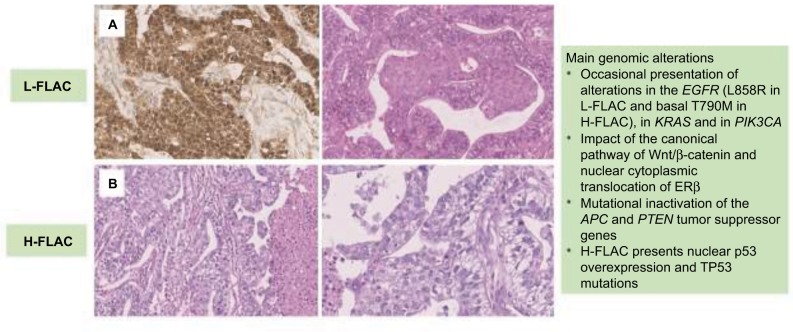
Fetal adenocarcinoma of the lung (FLAC) is a rare tumor. It accounts for ~0.1%-0.5% of all pulmonary neoplasms. Due to its rarity, much of the world literature regarding FLAC comes from case reports and case series. FLAC is an adenocarcinoma resembling developing fetal lung in its pseudoglandular stage (8-16 weeks of gestation). It is distinguishable from pulmonary blastoma (PB) because it lacks the mesenchymal component which is a hallmark finding in PB. Due to differences in histopathology and clinical course, FLAC has been further categorized into low-grade (L-FLAC) and high-grade (H-FLAC) forms. L-FLAC displays low nuclear atypia and prominent morule formation and has a pure pattern. H-FLAC typically presents with at least 50% fetal morphology, and is often associated with other conventional types of lung adenocarcinoma. FLAC expresses neuroendocrine markers and thyroid transcription factor 1 in most cases. L-FLAC has an aberrant nuclear/cytoplasmic expression of β-catenin and presents mutations in this gene. H-FLAC overexpresses p53. These tumors have a very low frequency of mutations in KRAS and EGFR; it is thought that they are different from a molecular point of view to conventional lung adenocarcinomas. Approximately 25%-40% of patients are asymptomatic at presentation; most of them are incidental findings on chest radiographs. H-FLAC is more common in elderly male patients, with a heavy smoking history. L-FLAC tends to occur in young females. Patients with L-FLAC are usually diagnosed with stage I-II disease, while patients with H-FLAC usually present with a more advanced-stage disease. Poor prognostic factors for FLAC are thoracic lymphadenopathy, metastases at diagnosis, and tumor recurrence; however, the 10-year survival for FLAC is estimated at 75%.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


