{"title":"Pre-hospital lung ultrasound for cardiac heart failure and COPD: is it worthwhile?","authors":"Mirko Zanatta, Piero Benato, Sigilfredo De Battisti, Concetta Pirozzi, Renato Ippolito, Vito Cianci","doi":"10.1186/s13089-018-0104-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pre-hospital ultrasound is a new challenge and lung ultrasound could be an interesting opportunity in the pre-hospital medical service. The aim of our study was to evaluate the efficacy of lung ultrasound in out-of-hospital non-traumatic respiratory insufficiency.</p><p><strong>Methods: </strong>We planned a case-controlled study in the ULSS 5 ovest vicentino area (Vicenza-Italy) enrolling subjects with severe dyspnea caused by cardiac heart failure or acute exacerbation of chronic obstructive pulmonary disease. We compared drugs administration, oxygen delivery, and laboratory tests between those patients with ultrasound integrated management and those without ultrasound.</p><p><strong>Results: </strong>Pre-hospital lung ultrasound had a high specificity (94.4%) and sensitivity (100%) for the correct identification of alveolar interstitial syndrome using B lines, whereas the percentages obtained with pleural effusion were lower (83.3, 53.3%, respectively). The patients with ultrasound integrated management received a more appropriate pharmacological therapy (p 0.01), as well as non-invasive ventilation (CPAP) was used more frequently in those with an acute exacerbation of chronic obstructive pulmonary disease (p 0.011). Laboratory tests and blood gases analysis were not significant different between the two study groups. In a sub-analysis of the patients with an A profile, we observed a significant lower concentration of PCO<sub>2</sub> in those with an ultrasound integrated management (PCO<sub>2</sub>: 42.62 vs 52.23 p 0.049). According with physicians' opinion, pre-hospital lung ultrasound gave important information or changed the therapy in the 42.3% of cases, whereas it just confirmed physical examination in the 67.7% of cases.</p><p><strong>Conclusions: </strong>Pre-hospital lung ultrasound is easy and feasible, and learning curve is rapid. Our study suggests that cardiac heart failure and acute exacerbation of chronic obstructive pulmonary disease can be considered two indications for pre-hospital ultrasound, and can improve the management of patient with acute respiratory insufficiency.</p>","PeriodicalId":46598,"journal":{"name":"Critical Ultrasound Journal","volume":"10 1","pages":"22"},"PeriodicalIF":3.6000,"publicationDate":"2018-09-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s13089-018-0104-5","citationCount":"15","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Ultrasound Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-018-0104-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 15
Abstract
Background: Pre-hospital ultrasound is a new challenge and lung ultrasound could be an interesting opportunity in the pre-hospital medical service. The aim of our study was to evaluate the efficacy of lung ultrasound in out-of-hospital non-traumatic respiratory insufficiency.
Methods: We planned a case-controlled study in the ULSS 5 ovest vicentino area (Vicenza-Italy) enrolling subjects with severe dyspnea caused by cardiac heart failure or acute exacerbation of chronic obstructive pulmonary disease. We compared drugs administration, oxygen delivery, and laboratory tests between those patients with ultrasound integrated management and those without ultrasound.
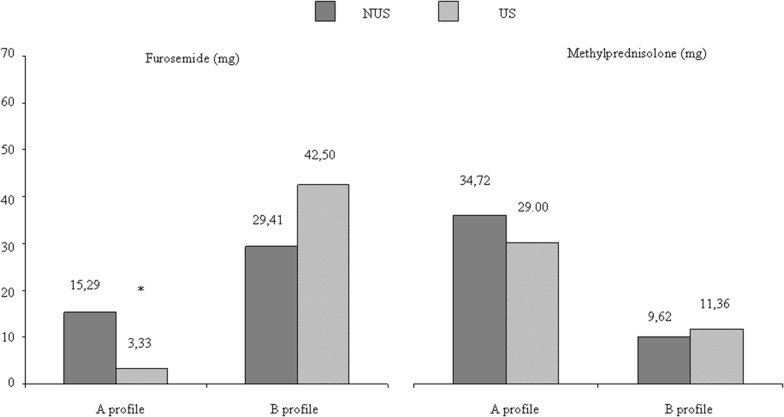
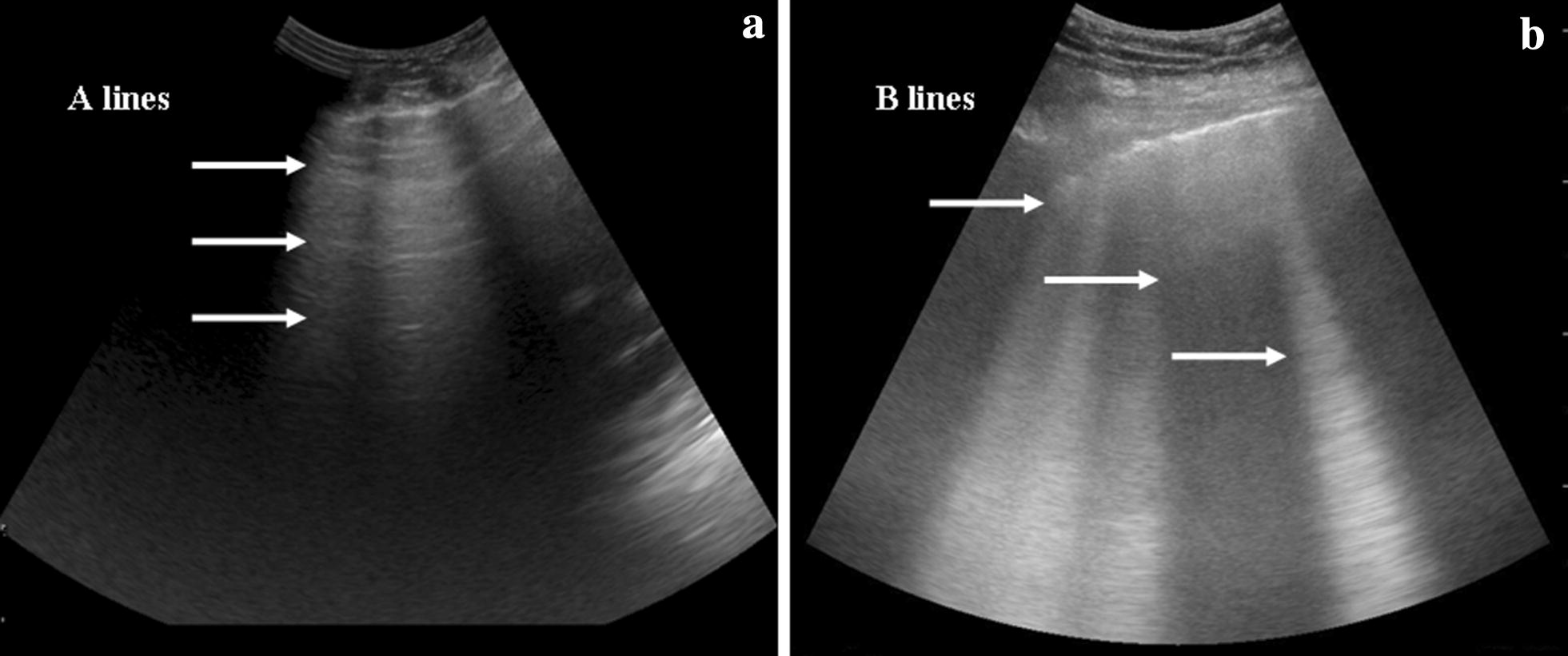
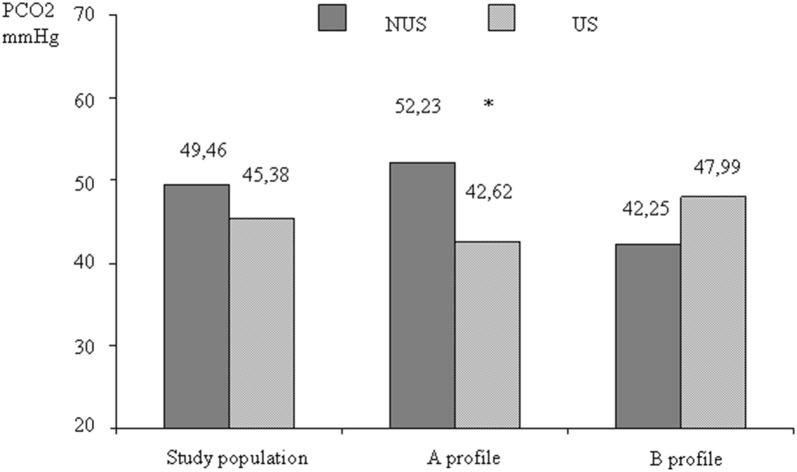
Results: Pre-hospital lung ultrasound had a high specificity (94.4%) and sensitivity (100%) for the correct identification of alveolar interstitial syndrome using B lines, whereas the percentages obtained with pleural effusion were lower (83.3, 53.3%, respectively). The patients with ultrasound integrated management received a more appropriate pharmacological therapy (p 0.01), as well as non-invasive ventilation (CPAP) was used more frequently in those with an acute exacerbation of chronic obstructive pulmonary disease (p 0.011). Laboratory tests and blood gases analysis were not significant different between the two study groups. In a sub-analysis of the patients with an A profile, we observed a significant lower concentration of PCO2 in those with an ultrasound integrated management (PCO2: 42.62 vs 52.23 p 0.049). According with physicians' opinion, pre-hospital lung ultrasound gave important information or changed the therapy in the 42.3% of cases, whereas it just confirmed physical examination in the 67.7% of cases.
Conclusions: Pre-hospital lung ultrasound is easy and feasible, and learning curve is rapid. Our study suggests that cardiac heart failure and acute exacerbation of chronic obstructive pulmonary disease can be considered two indications for pre-hospital ultrasound, and can improve the management of patient with acute respiratory insufficiency.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


