Kelsey H Collins, Behnam Sharif, Raylene A Reimer, Claudia Sanmartin, Walter Herzog, Rick Chin, Deborah A Marshall
{"title":"Association of Metabolic Markers with self-reported osteoarthritis among middle-aged BMI-defined non-obese individuals: a cross-sectional study.","authors":"Kelsey H Collins, Behnam Sharif, Raylene A Reimer, Claudia Sanmartin, Walter Herzog, Rick Chin, Deborah A Marshall","doi":"10.1186/s40608-018-0201-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Osteoarthritis (OA) is a chronic degenerative joint disease. While it is well-established that obesity affects OA through increased axial loading on the joint cartilage, the indirect effect of obesity through metabolic processes among the body mass index (BMI)-defined non-obese population, i.e., BMI < 30 kg/m<sup>2</sup>, is less known. Our goal was to evaluate the association of metabolic markers including body fat percentage (BF%), waist circumference, maximum weight gain during adulthood and serum creatinine with self-reported OA to establish if such measures offer additional information over BMI among the non-obese population between 40 and 65 years of age.</p><p><strong>Methods: </strong>Cross-sectional data from two cycles of the Canadian Health Measures Survey (CHMS) in 2007-2009 and 2009-2011 were analyzed. Sex-specific logistic regression models were developed to evaluate the association of self-reported OA with metabolic markers. Models were separately adjusted for age, BMI categories and serum creatinine, and a stratified analysis across BM categories was performed. In a secondary analysis, we evaluated the association of self-reported OA, cardiovascular diseases and hypertension across BF% categories.</p><p><strong>Results: </strong>Of 2462 individuals, 217 (8.8%) self-reported OA. After adjusting for age and BMI, those within BF%-defined overweight/obese category had 2.67 (95% CI: 1.32-3.51) and 2.11(95% CI: 1.38-3.21) times higher odds of reporting self-reported OA compared to those within BF%-defined athletic/acceptable category for females and males, respectively. BF% was also significantly associated with self-reported OA after adjusting for age and serum creatinine only among females (OR: 1.47, 95%CI: 1.12-1.84). Furthermore, among the BMI-defined overweight group, the age-adjusted odds of self-reported OA was significantly higher for overweight/obese BF% compared to athletic/acceptable BF% in both females and males. In a secondary analysis, we showed that the association of self-reported OA and hypertension/cardiovascular diseases is significantly higher among BF% overweight/obese (OR: 1.37, 95%CI: 1.19-3.09) compared to BF% athletic/acceptable (OR: 1.13, 95%CI: 0.87-2.82).</p><p><strong>Conclusion: </strong>Our results provide corroborating evidence for a relationship between body fat and OA in a population-based study, while no significant independent correlates were found between other metabolic markers and OA prevalence. Future investigation on the longitudinal relationship between BF and OA among this sub-population may inform targeted prevention opportunities.</p>","PeriodicalId":37440,"journal":{"name":"BMC Obesity","volume":"5 ","pages":"23"},"PeriodicalIF":0.0000,"publicationDate":"2018-09-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6120068/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Obesity","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40608-018-0201-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Osteoarthritis (OA) is a chronic degenerative joint disease. While it is well-established that obesity affects OA through increased axial loading on the joint cartilage, the indirect effect of obesity through metabolic processes among the body mass index (BMI)-defined non-obese population, i.e., BMI < 30 kg/m2, is less known. Our goal was to evaluate the association of metabolic markers including body fat percentage (BF%), waist circumference, maximum weight gain during adulthood and serum creatinine with self-reported OA to establish if such measures offer additional information over BMI among the non-obese population between 40 and 65 years of age.
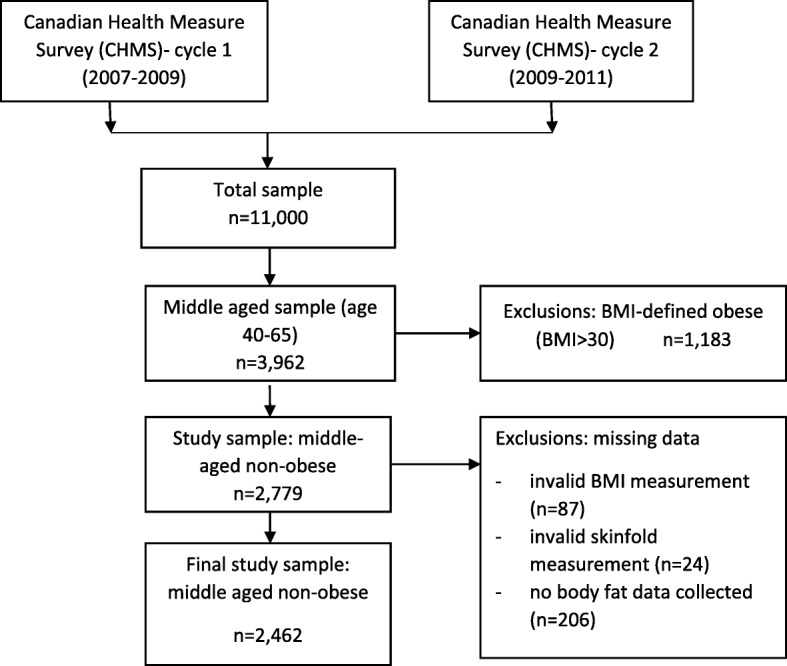
Methods: Cross-sectional data from two cycles of the Canadian Health Measures Survey (CHMS) in 2007-2009 and 2009-2011 were analyzed. Sex-specific logistic regression models were developed to evaluate the association of self-reported OA with metabolic markers. Models were separately adjusted for age, BMI categories and serum creatinine, and a stratified analysis across BM categories was performed. In a secondary analysis, we evaluated the association of self-reported OA, cardiovascular diseases and hypertension across BF% categories.
Results: Of 2462 individuals, 217 (8.8%) self-reported OA. After adjusting for age and BMI, those within BF%-defined overweight/obese category had 2.67 (95% CI: 1.32-3.51) and 2.11(95% CI: 1.38-3.21) times higher odds of reporting self-reported OA compared to those within BF%-defined athletic/acceptable category for females and males, respectively. BF% was also significantly associated with self-reported OA after adjusting for age and serum creatinine only among females (OR: 1.47, 95%CI: 1.12-1.84). Furthermore, among the BMI-defined overweight group, the age-adjusted odds of self-reported OA was significantly higher for overweight/obese BF% compared to athletic/acceptable BF% in both females and males. In a secondary analysis, we showed that the association of self-reported OA and hypertension/cardiovascular diseases is significantly higher among BF% overweight/obese (OR: 1.37, 95%CI: 1.19-3.09) compared to BF% athletic/acceptable (OR: 1.13, 95%CI: 0.87-2.82).
Conclusion: Our results provide corroborating evidence for a relationship between body fat and OA in a population-based study, while no significant independent correlates were found between other metabolic markers and OA prevalence. Future investigation on the longitudinal relationship between BF and OA among this sub-population may inform targeted prevention opportunities.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


