Luciano Rodrigo Peres, Matheus Silva Teixeira, Caetano Scalizi Júnior, Wolf Akl Filho
{"title":"Radiological evaluation of the femoral tunnel positioning in anterior cruciate ligament reconstruction","authors":"Luciano Rodrigo Peres, Matheus Silva Teixeira, Caetano Scalizi Júnior, Wolf Akl Filho","doi":"10.1016/j.rboe.2018.05.001","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><p>To evaluate the inclination and the length of the femoral tunnel in patients submitted to anterior cruciate ligament reconstruction (ACL) surgery by transtibial and anatomical techniques.</p></div><div><h3>Methods</h3><p>This is an analytical observational study in patients with ACL injury that underwent arthroscopic reconstruction through transtibial and anatomical surgical techniques. In the immediate postoperative period, computed tomography (CT) and anteroposterior (AP) view digital radiographs (X-rays) were performed to evaluate the inclination and length of the femoral tunnel.</p></div><div><h3>Results</h3><p>Forty-two patients were analyzed: 27 underwent anatomical reconstruction and 15, transtibial reconstruction. The inclination angle and tunnel length by the transtibial technique are always greater than by the anatomical technique. The mean inclination angles were 59.75° (53.9–66.1°) in the X-rays and 54.17° (43.5–62.3°) in CT for the transtibial technique, and 42.91° (29.3–57.4°) in the X-rays and 39.10° (23.8–50.6°) in CT for the anatomical technique. Regarding the length of the femoral tunnel, the transtibial technique promotes longer tunnels: mean 55.7<!--> <!-->mm (40.0–70.2<!--> <!-->mm) in the transtibial and 35.5<!--> <!-->mm (24.5–47<!--> <!-->mm) in the anatomical technique. No statistically significant correlation was observed between the length and the inclination of the tunnel, regardless of the technique used. Thus, these variables can be considered as independent.</p></div><div><h3>Conclusion</h3><p>The anatomical reconstruction technique presented shorter femoral tunnels and lower angle of inclination than the transtibial technique. The CT showed smaller inclination angle than the X-rays, regardless of the surgical technique.</p></div>","PeriodicalId":101095,"journal":{"name":"Revista Brasileira de Ortopedia (English Edition)","volume":"53 4","pages":"Pages 397-403"},"PeriodicalIF":0.0000,"publicationDate":"2018-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1016/j.rboe.2018.05.001","citationCount":"5","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Revista Brasileira de Ortopedia (English Edition)","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2255497118300661","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 5
Abstract
Objective
To evaluate the inclination and the length of the femoral tunnel in patients submitted to anterior cruciate ligament reconstruction (ACL) surgery by transtibial and anatomical techniques.
Methods
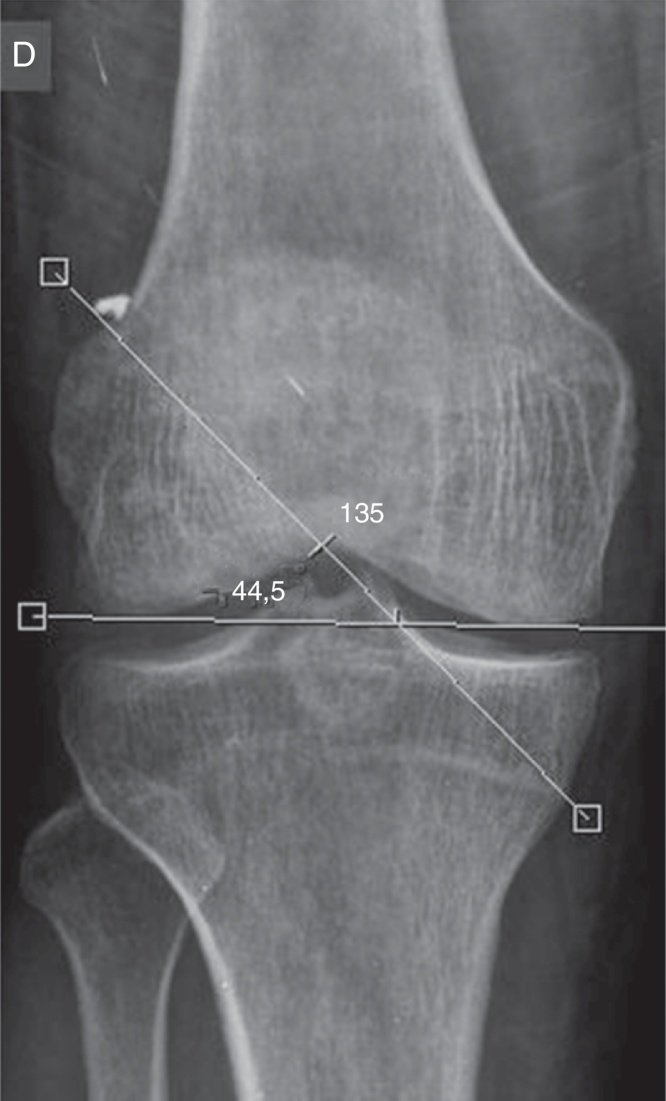
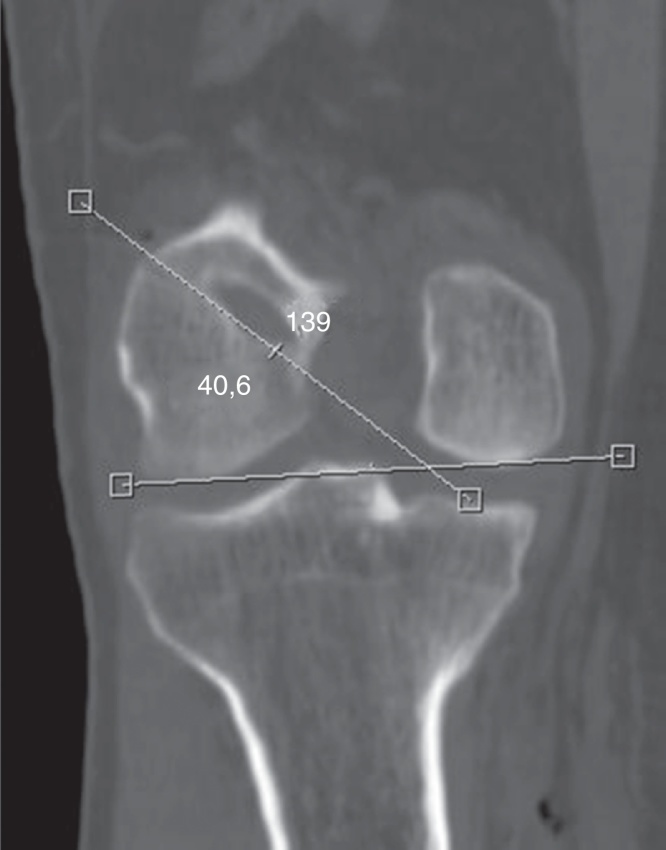
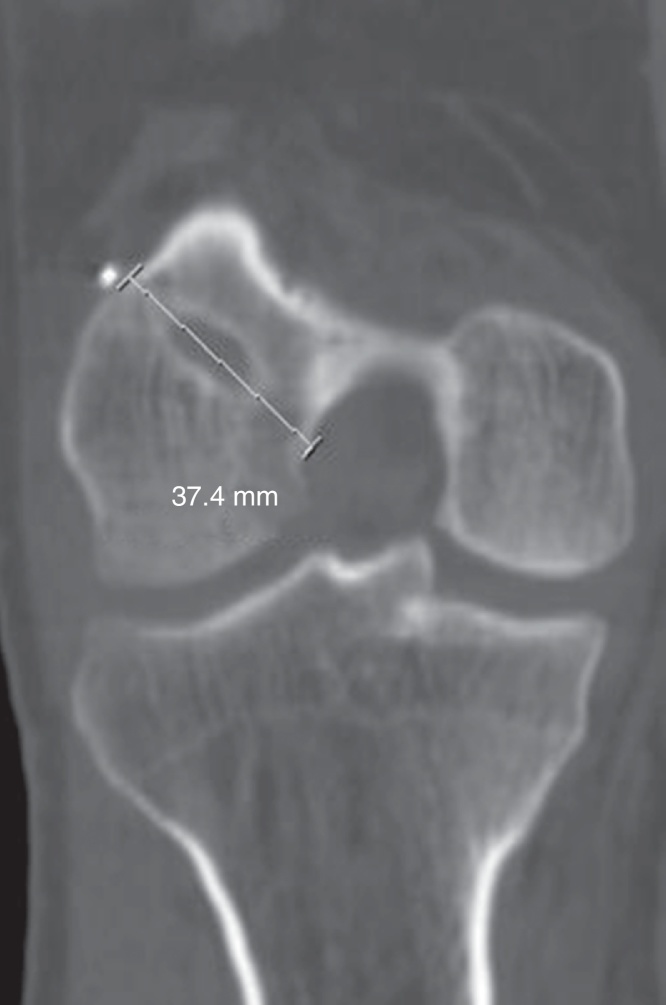
This is an analytical observational study in patients with ACL injury that underwent arthroscopic reconstruction through transtibial and anatomical surgical techniques. In the immediate postoperative period, computed tomography (CT) and anteroposterior (AP) view digital radiographs (X-rays) were performed to evaluate the inclination and length of the femoral tunnel.
Results
Forty-two patients were analyzed: 27 underwent anatomical reconstruction and 15, transtibial reconstruction. The inclination angle and tunnel length by the transtibial technique are always greater than by the anatomical technique. The mean inclination angles were 59.75° (53.9–66.1°) in the X-rays and 54.17° (43.5–62.3°) in CT for the transtibial technique, and 42.91° (29.3–57.4°) in the X-rays and 39.10° (23.8–50.6°) in CT for the anatomical technique. Regarding the length of the femoral tunnel, the transtibial technique promotes longer tunnels: mean 55.7 mm (40.0–70.2 mm) in the transtibial and 35.5 mm (24.5–47 mm) in the anatomical technique. No statistically significant correlation was observed between the length and the inclination of the tunnel, regardless of the technique used. Thus, these variables can be considered as independent.
Conclusion
The anatomical reconstruction technique presented shorter femoral tunnels and lower angle of inclination than the transtibial technique. The CT showed smaller inclination angle than the X-rays, regardless of the surgical technique.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


