Michael M Segal, Alanna K Rahm, Nathan C Hulse, Grant Wood, Janet L Williams, Lynn Feldman, Gregory J Moore, David Gehrum, Michelle Yefko, Steven Mayernick, Roger Gildersleeve, Margie C Sunderland, Steven B Bleyl, Peter Haug, Marc S Williams
{"title":"Experience with Integrating Diagnostic Decision Support Software with Electronic Health Records: Benefits versus Risks of Information Sharing.","authors":"Michael M Segal, Alanna K Rahm, Nathan C Hulse, Grant Wood, Janet L Williams, Lynn Feldman, Gregory J Moore, David Gehrum, Michelle Yefko, Steven Mayernick, Roger Gildersleeve, Margie C Sunderland, Steven B Bleyl, Peter Haug, Marc S Williams","doi":"10.5334/egems.244","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Reducing misdiagnosis has long been a goal of medical informatics. Current thinking has focused on achieving this goal by integrating diagnostic decision support into electronic health records.</p><p><strong>Methods: </strong>A diagnostic decision support system already in clinical use was integrated into electronic health record systems at two large health systems, after clinician input on desired capabilities. The decision support provided three outputs: editable text for use in a clinical note, a summary including the suggested differential diagnosis with a graphical representation of probability, and a list of pertinent positive and pertinent negative findings (with onsets).</p><p><strong>Results: </strong>Structured interviews showed widespread agreement that the tool was useful and that the integration improved workflow. There was disagreement among various specialties over the risks versus benefits of documenting intermediate diagnostic thinking. Benefits were most valued by specialists involved in diagnostic testing, who were able to use the additional clinical context for richer interpretation of test results. Risks were most cited by physicians making clinical diagnoses, who expressed concern that a process that generated diagnostic possibilities exposed them to legal liability.</p><p><strong>Discussion and conclusion: </strong>Reconciling the preferences of the various groups could include saving only the finding list as a patient-wide resource, saving intermediate diagnostic thinking only temporarily, or adoption of professional guidelines to clarify the role of decision support in diagnosis.</p>","PeriodicalId":72880,"journal":{"name":"EGEMS (Washington, DC)","volume":"5 1","pages":"23"},"PeriodicalIF":0.0000,"publicationDate":"2017-12-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d9/2d/egems-5-1-244.PMC5994959.pdf","citationCount":"13","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"EGEMS (Washington, DC)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5334/egems.244","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 13
Abstract
Introduction: Reducing misdiagnosis has long been a goal of medical informatics. Current thinking has focused on achieving this goal by integrating diagnostic decision support into electronic health records.
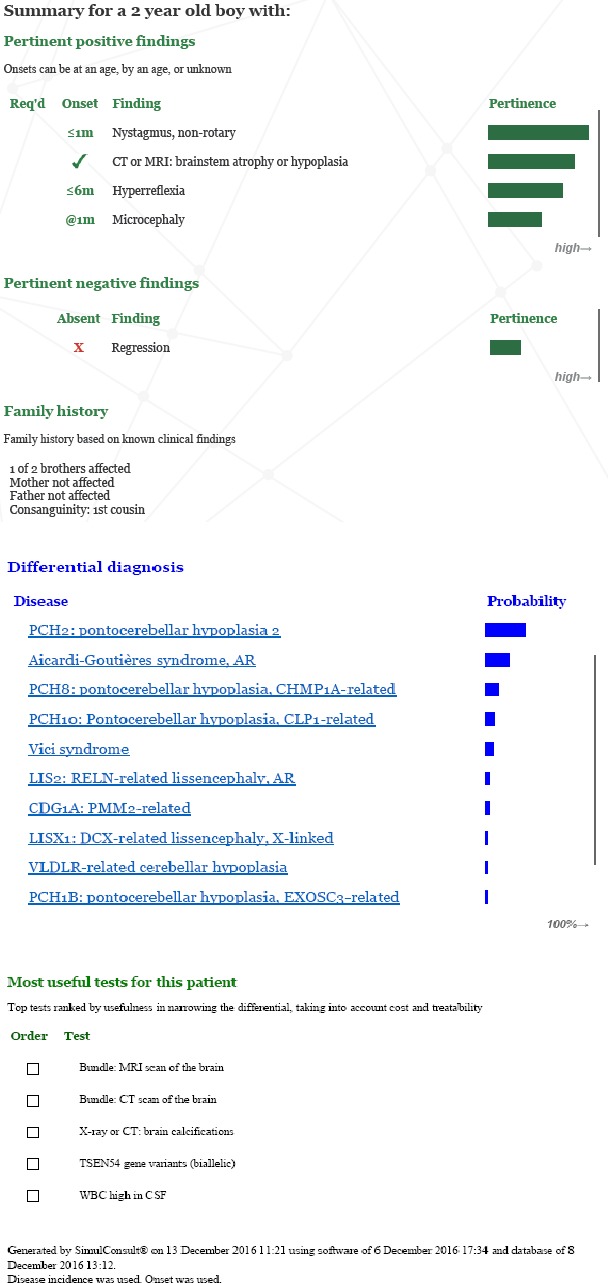
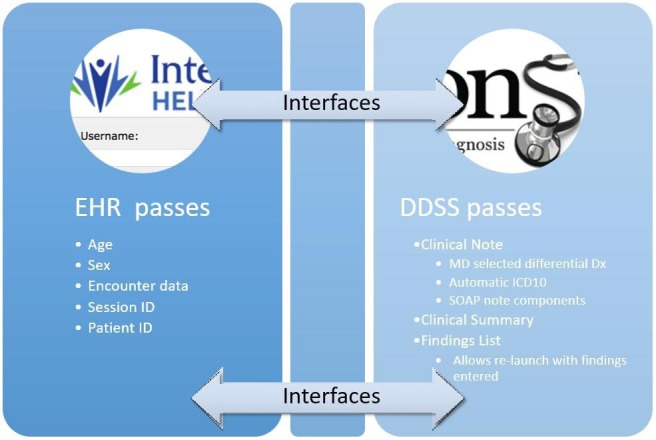
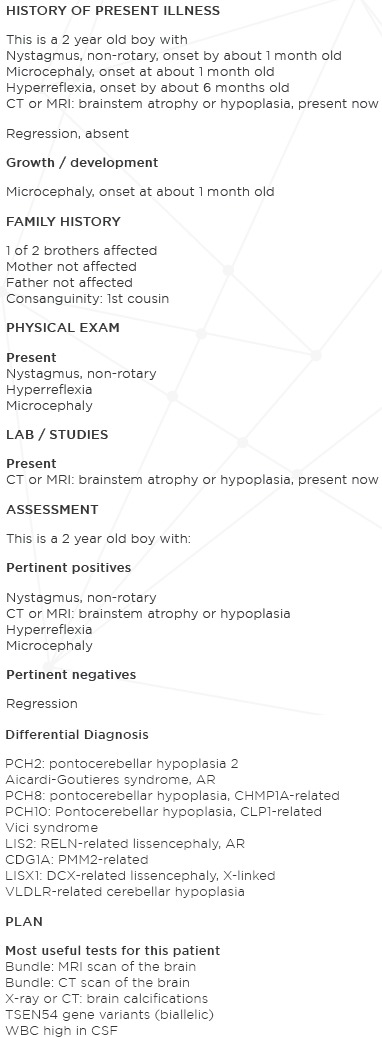
Methods: A diagnostic decision support system already in clinical use was integrated into electronic health record systems at two large health systems, after clinician input on desired capabilities. The decision support provided three outputs: editable text for use in a clinical note, a summary including the suggested differential diagnosis with a graphical representation of probability, and a list of pertinent positive and pertinent negative findings (with onsets).
Results: Structured interviews showed widespread agreement that the tool was useful and that the integration improved workflow. There was disagreement among various specialties over the risks versus benefits of documenting intermediate diagnostic thinking. Benefits were most valued by specialists involved in diagnostic testing, who were able to use the additional clinical context for richer interpretation of test results. Risks were most cited by physicians making clinical diagnoses, who expressed concern that a process that generated diagnostic possibilities exposed them to legal liability.
Discussion and conclusion: Reconciling the preferences of the various groups could include saving only the finding list as a patient-wide resource, saving intermediate diagnostic thinking only temporarily, or adoption of professional guidelines to clarify the role of decision support in diagnosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


