{"title":"The effect of passive leg-raising maneuver on hemodynamic stability during anesthesia induction for adult cardiac surgery.","authors":"Solmaz Fakhari, Eissa Bilehjani, Haleh Farzin, Hojjat Pourfathi, Mohsen Chalabianlou","doi":"10.2147/IBPC.S126514","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Some cardiac patients do not tolerate the intravenous fluid load commonly administered before anesthesia induction. This study investigated preinduction passive leg-raising maneuver (PLRM) as an alternative method to fluid loading before cardiac anesthesia.</p><p><strong>Methods and materials: </strong>During a 6-month period, 120 adult elective heart surgery patients were enrolled in this study and allocated into 2 groups: PLRM group vs control group (n=60). Anesthesia was induced using midazolam, fentanyl, and cisatracurium. Initially, 250 mL of fluid was administrated intravenously in all of patients before anesthesia induction. Then in the PLRM group, PLRM was performed starting 2 minutes before anesthesia induction and continued for 20 minutes after tracheal intubation. In the control group, anesthesia was induced in a simple supine position. Heart rate, invasive mean arterial blood pressure (MAP), and central venous pressure (CVP) were recorded before PLRM, before anesthetic induction, before laryngoscopy, and at 5, 10, and 20 minutes after tracheal intubation. The hypotension episode rate (MAP <70 mmHg) and CVP changes were compared between the 2 groups. The predictive value of the ≥3 mmHg increase in CVP value in response to PLRM for hypotension prevention was defined.</p><p><strong>Results: </strong>Hypotension rates were lower in the PLRM group (63.3% vs 81.6%; <i>P</i>-value 0.04), and MAP was higher among PLRM patients immediately before anesthetic injection, before laryngoscopy, and 20 minutes after intubation, compared to the control group. PLRM increased CVP by 3.57±4.9 mmHg (from 7.50±2.94 to 11.05±3.55 mmHg), which required several minutes to reach peak value, returning to baseline after 15 minutes. This change did not correlate to subsequent MAP changes; an increase in the CVP value ≥3 mmHg decreased the postinduction hypotension rate by 62.50%.</p><p><strong>Conclusion: </strong>Preinduction PLRM can provide a more stable hemodynamic status in adult cardiac surgery patients and decreases anesthesia-induced hypotension rates by 62.50%. Rate of the changes in the CVP value caused by PLRM is not predictive of subsequent MAP changes.</p>","PeriodicalId":45299,"journal":{"name":"Integrated Blood Pressure Control","volume":"11 ","pages":"57-63"},"PeriodicalIF":2.7000,"publicationDate":"2018-06-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.2147/IBPC.S126514","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Integrated Blood Pressure Control","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/IBPC.S126514","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 4
Abstract
Introduction: Some cardiac patients do not tolerate the intravenous fluid load commonly administered before anesthesia induction. This study investigated preinduction passive leg-raising maneuver (PLRM) as an alternative method to fluid loading before cardiac anesthesia.
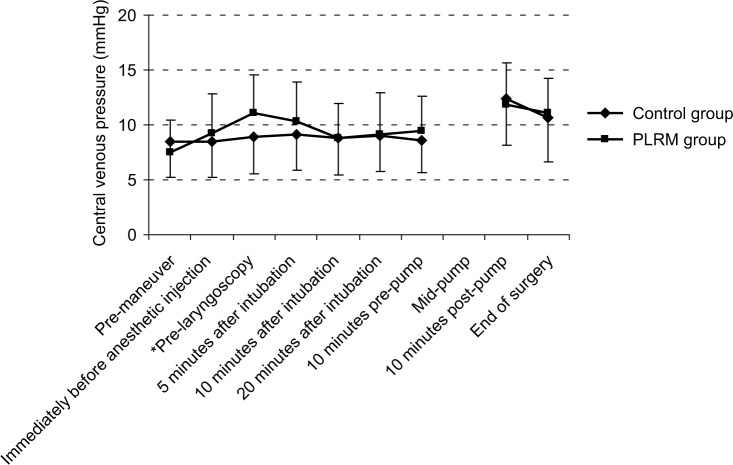
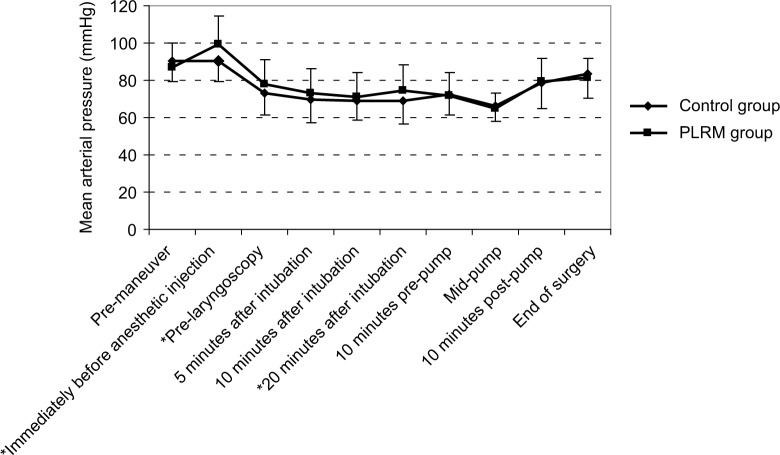
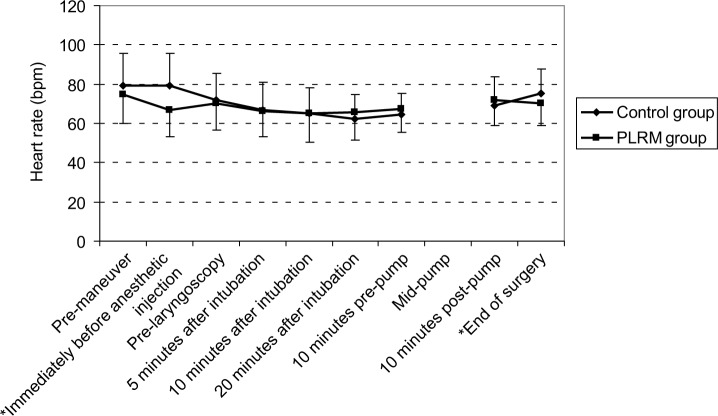
Methods and materials: During a 6-month period, 120 adult elective heart surgery patients were enrolled in this study and allocated into 2 groups: PLRM group vs control group (n=60). Anesthesia was induced using midazolam, fentanyl, and cisatracurium. Initially, 250 mL of fluid was administrated intravenously in all of patients before anesthesia induction. Then in the PLRM group, PLRM was performed starting 2 minutes before anesthesia induction and continued for 20 minutes after tracheal intubation. In the control group, anesthesia was induced in a simple supine position. Heart rate, invasive mean arterial blood pressure (MAP), and central venous pressure (CVP) were recorded before PLRM, before anesthetic induction, before laryngoscopy, and at 5, 10, and 20 minutes after tracheal intubation. The hypotension episode rate (MAP <70 mmHg) and CVP changes were compared between the 2 groups. The predictive value of the ≥3 mmHg increase in CVP value in response to PLRM for hypotension prevention was defined.
Results: Hypotension rates were lower in the PLRM group (63.3% vs 81.6%; P-value 0.04), and MAP was higher among PLRM patients immediately before anesthetic injection, before laryngoscopy, and 20 minutes after intubation, compared to the control group. PLRM increased CVP by 3.57±4.9 mmHg (from 7.50±2.94 to 11.05±3.55 mmHg), which required several minutes to reach peak value, returning to baseline after 15 minutes. This change did not correlate to subsequent MAP changes; an increase in the CVP value ≥3 mmHg decreased the postinduction hypotension rate by 62.50%.
Conclusion: Preinduction PLRM can provide a more stable hemodynamic status in adult cardiac surgery patients and decreases anesthesia-induced hypotension rates by 62.50%. Rate of the changes in the CVP value caused by PLRM is not predictive of subsequent MAP changes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


