Lucas W Thornblade, David R Flum, Abraham D Flaxman
{"title":"Predicting Future Elective Colon Resection for Diverticulitis Using Patterns of Health Care Utilization.","authors":"Lucas W Thornblade, David R Flum, Abraham D Flaxman","doi":"10.5334/egems.193","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Recurrent diverticulitis is the most common reason for elective colon surgery and, although professional societies now recommend against early resection, its use continues to rise. Shared decision making decreases use of low-value surgery but identifying which patients are most likely to elect surgery has proven difficult. We hypothesized that Machine Learning algorithms using health care utilization (HCU) data can predict future clinical events including early resection for diverticulitis.</p><p><strong>Study design: </strong>We developed models for predicting future surgery among patients with new diagnoses of diverticulitis (2009-2012) from the MarketScan® database. Claims data (diagnosis, procedural, and drug codes) were used to train three Machine Learning algorithms to predict surgery occurring between 52 and 104 weeks following diagnosis.</p><p><strong>Results: </strong>Of 82,231 patients with incident diverticulitis (age 51 ± 8 years, 52% female), 1.2% went on to elective colon resection. Using maximal training data (152 consecutive weeks of claims), the Gradient Boosting Machine model predicted elective surgery with an area under the curve (AUC) of 75% (95% uncertainty interval [UI] 71-79%). Models trained on less data resulted in less accurate prediction (AUC: 68% [64-74%] using 128 weeks, 57% [53-63%] using 104 weeks). The majority of resections (85%) were identified as low-value.</p><p><strong>Conclusion: </strong>By applying Machine Learning to HCU data from the time around a diagnosis of diverticulitis, we predicted elective surgery weeks to months in advance, with moderate accuracy. Identifying patients who are most likely to elect surgery for diverticulitis provides an opportunity for effective shared decision making initiatives aimed at reducing the use of costly low-value care.</p>","PeriodicalId":72880,"journal":{"name":"EGEMS (Washington, DC)","volume":" ","pages":"1"},"PeriodicalIF":0.0000,"publicationDate":"2018-01-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5983027/pdf/","citationCount":"7","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"EGEMS (Washington, DC)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5334/egems.193","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 7
Abstract
Background: Recurrent diverticulitis is the most common reason for elective colon surgery and, although professional societies now recommend against early resection, its use continues to rise. Shared decision making decreases use of low-value surgery but identifying which patients are most likely to elect surgery has proven difficult. We hypothesized that Machine Learning algorithms using health care utilization (HCU) data can predict future clinical events including early resection for diverticulitis.
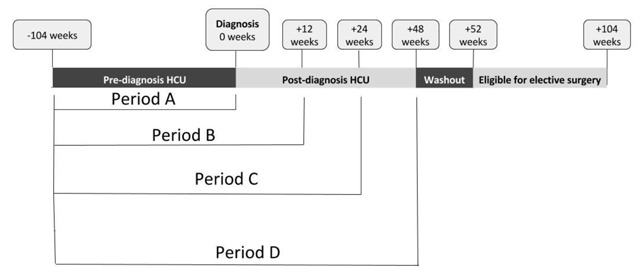
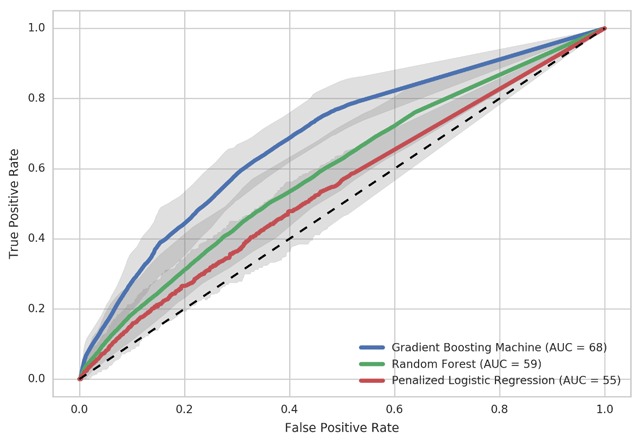
Study design: We developed models for predicting future surgery among patients with new diagnoses of diverticulitis (2009-2012) from the MarketScan® database. Claims data (diagnosis, procedural, and drug codes) were used to train three Machine Learning algorithms to predict surgery occurring between 52 and 104 weeks following diagnosis.
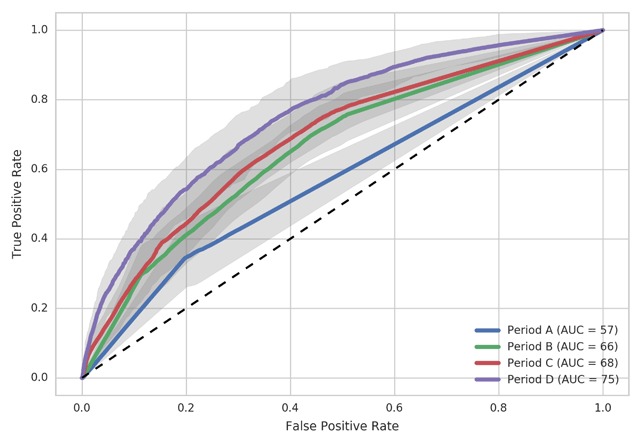
Results: Of 82,231 patients with incident diverticulitis (age 51 ± 8 years, 52% female), 1.2% went on to elective colon resection. Using maximal training data (152 consecutive weeks of claims), the Gradient Boosting Machine model predicted elective surgery with an area under the curve (AUC) of 75% (95% uncertainty interval [UI] 71-79%). Models trained on less data resulted in less accurate prediction (AUC: 68% [64-74%] using 128 weeks, 57% [53-63%] using 104 weeks). The majority of resections (85%) were identified as low-value.
Conclusion: By applying Machine Learning to HCU data from the time around a diagnosis of diverticulitis, we predicted elective surgery weeks to months in advance, with moderate accuracy. Identifying patients who are most likely to elect surgery for diverticulitis provides an opportunity for effective shared decision making initiatives aimed at reducing the use of costly low-value care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


