Genna R Cohen, David J Jones, Jessica Heeringa, Kirsten Barrett, Michael F Furukawa, Dan Miller, Anne Mutti, James D Reschovsky, Rachel Machta, Stephen M Shortell, Taressa Fraze, Eugene Rich
{"title":"Leveraging Diverse Data Sources to Identify and Describe U.S. Health Care Delivery Systems.","authors":"Genna R Cohen, David J Jones, Jessica Heeringa, Kirsten Barrett, Michael F Furukawa, Dan Miller, Anne Mutti, James D Reschovsky, Rachel Machta, Stephen M Shortell, Taressa Fraze, Eugene Rich","doi":"10.5334/egems.200","DOIUrl":null,"url":null,"abstract":"<p><p>Health care delivery systems are a growing presence in the U.S., yet research is hindered by the lack of universally agreed-upon criteria to denote formal systems. A clearer understanding of how to leverage real-world data sources to empirically identify systems is a necessary first step to such policy-relevant research. We draw from our experience in the Agency for Healthcare Research and Quality's Comparative Health System Performance (CHSP) initiative to assess available data sources to identify and describe systems, including system members (for example, hospitals and physicians) and relationships among the members (for example, hospital ownership of physician groups). We highlight five national data sources that either explicitly track system membership or detail system relationships: (1) American Hospital Association annual survey of hospitals; (2) Healthcare Relational Services Databases; (3) SK&A Healthcare Databases; (4) Provider Enrollment, Chain, and Ownership System; and (5) Internal Revenue Service 990 forms. Each data source has strengths and limitations for identifying and describing systems due to their varied content, linkages across data sources, and data collection methods. In addition, although no single national data source provides a complete picture of U.S. systems and their members, the CHSP initiative will create an early model of how such data can be combined to compensate for their individual limitations. Identifying systems in a way that can be repeated over time and linked to a host of other data sources will support analysis of how different types of organizations deliver health care and, ultimately, comparison of their performance.</p>","PeriodicalId":72880,"journal":{"name":"EGEMS (Washington, DC)","volume":"5 3","pages":"9"},"PeriodicalIF":0.0000,"publicationDate":"2017-12-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5983023/pdf/","citationCount":"17","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"EGEMS (Washington, DC)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5334/egems.200","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 17
Abstract
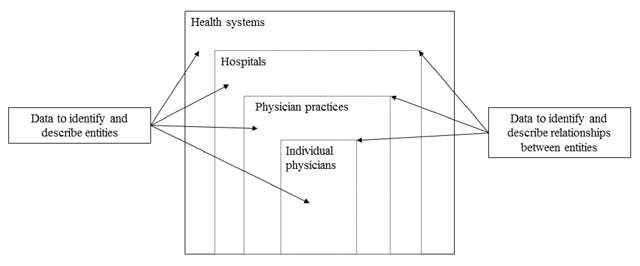
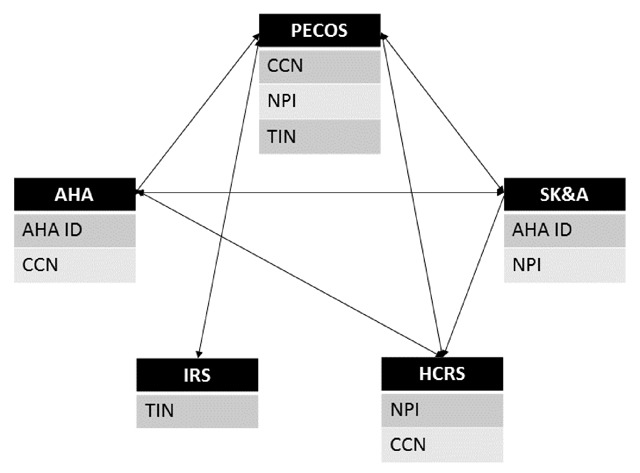
Health care delivery systems are a growing presence in the U.S., yet research is hindered by the lack of universally agreed-upon criteria to denote formal systems. A clearer understanding of how to leverage real-world data sources to empirically identify systems is a necessary first step to such policy-relevant research. We draw from our experience in the Agency for Healthcare Research and Quality's Comparative Health System Performance (CHSP) initiative to assess available data sources to identify and describe systems, including system members (for example, hospitals and physicians) and relationships among the members (for example, hospital ownership of physician groups). We highlight five national data sources that either explicitly track system membership or detail system relationships: (1) American Hospital Association annual survey of hospitals; (2) Healthcare Relational Services Databases; (3) SK&A Healthcare Databases; (4) Provider Enrollment, Chain, and Ownership System; and (5) Internal Revenue Service 990 forms. Each data source has strengths and limitations for identifying and describing systems due to their varied content, linkages across data sources, and data collection methods. In addition, although no single national data source provides a complete picture of U.S. systems and their members, the CHSP initiative will create an early model of how such data can be combined to compensate for their individual limitations. Identifying systems in a way that can be repeated over time and linked to a host of other data sources will support analysis of how different types of organizations deliver health care and, ultimately, comparison of their performance.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


