{"title":"Intraoperative Gastric Tube Intubation: A Summary of Case Studies and Review of the Literature.","authors":"Michael Long, Melissa Machan, Luis Tollinche","doi":"10.4236/ojanes.2017.73005","DOIUrl":null,"url":null,"abstract":"<p><strong>Study objective: </strong>Establish complications and risk factors that are associated with blind tube insertion, evaluate the validity of correct placement verification methods, establish the rationales supporting its employment by anesthesia providers, and describe various deployment facilitators described in current literature.</p><p><strong>Measurements: </strong>An exhaustive literature review of the databases Medline, CINAHL, Cochrane Collaboration, Scopus, and Google Scholar was performed applying the search terms \"gastric tube\", \"complications\", \"decompression\", \"blind insertion\", \"perioperative\", \"intraoperative\" in various order sequences. A five-year limit was applied to limit the number and timeliness of articles selected.</p><p><strong>Main results: </strong>Patients are exposed to potentially serious morbidity and mortality from blindly inserted gastric tubes. Risk factors associated with malposition include blind insertion, the presence of endotracheal tubes, altered sensorium, and previous tube misplacements. Pulmonary aspiration risk prevention remains the only indication for anesthesia-related intraoperative use. There are no singularly effective tools that predict or verify the proper placement of blindly inserted gastric tubes. Current placement facilitation techniques are perpetuated through anecdotal experience and technique variability warrants further study.</p><p><strong>Conclusion: </strong>In the absence of aspiration risk factors or the need for surgical decompression in ASA classification I & II patients, a moratorium should be instituted on the elective use of gastric tubes.</p>","PeriodicalId":56551,"journal":{"name":"麻醉学期刊(英文)","volume":"7 3","pages":"43-62"},"PeriodicalIF":0.0000,"publicationDate":"2017-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4236/ojanes.2017.73005","citationCount":"9","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"麻醉学期刊(英文)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4236/ojanes.2017.73005","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 9
Abstract
Study objective: Establish complications and risk factors that are associated with blind tube insertion, evaluate the validity of correct placement verification methods, establish the rationales supporting its employment by anesthesia providers, and describe various deployment facilitators described in current literature.
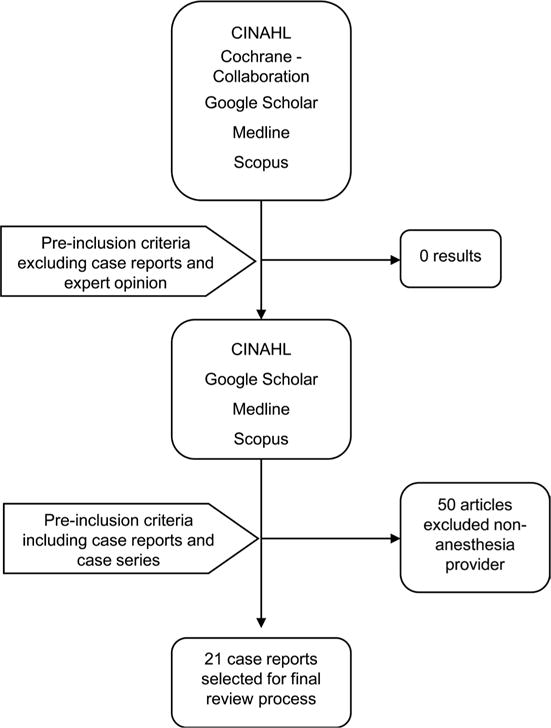
Measurements: An exhaustive literature review of the databases Medline, CINAHL, Cochrane Collaboration, Scopus, and Google Scholar was performed applying the search terms "gastric tube", "complications", "decompression", "blind insertion", "perioperative", "intraoperative" in various order sequences. A five-year limit was applied to limit the number and timeliness of articles selected.
Main results: Patients are exposed to potentially serious morbidity and mortality from blindly inserted gastric tubes. Risk factors associated with malposition include blind insertion, the presence of endotracheal tubes, altered sensorium, and previous tube misplacements. Pulmonary aspiration risk prevention remains the only indication for anesthesia-related intraoperative use. There are no singularly effective tools that predict or verify the proper placement of blindly inserted gastric tubes. Current placement facilitation techniques are perpetuated through anecdotal experience and technique variability warrants further study.
Conclusion: In the absence of aspiration risk factors or the need for surgical decompression in ASA classification I & II patients, a moratorium should be instituted on the elective use of gastric tubes.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


