{"title":"Universal Rapid Human Immunodeficiency Virus Screening at Delivery: A Cost-Effectiveness Analysis.","authors":"Rachel K Scott, Stacia Crochet, Chun-Chih Huang","doi":"10.1155/2018/6024698","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To determine the cost-effectiveness of universal maternal HIV screening at time of delivery to decrease mother-to-child transmission (MTCT), by comparing the cost and quality-adjusted life years (QALYs) of universal rapid HIV screening at time of delivery to two current standards of care for prenatal HIV screening in the United States.</p><p><strong>Study design: </strong>We conducted a cost-effectiveness analysis to compare the cost and QALY of universal intrapartum rapid HIV screening with two current standards of care: (I) opt-out rapid HIV testing limited to patients without previous third-trimester screening and (II) opt-out rapid HIV testing limited to patients without any prenatal screening. We developed a decision-tree model and performed sensitivity analyses to estimate the impact of variances in QALY, estimated lifetime medical costs, HIV prevalence, and cumulative incidence.</p><p><strong>Results: </strong>The incremental cost-effectiveness ratio for universal screening was $7,973.45/QALY. The results remained robust to sensitivity analysis, except for annual cumulative incidence. In areas with an annual cumulative incidence rate of <0.02% for reproductive-age women, the incremental cost-effectiveness ratio for the expanded program would exceed $89,926.94/QALY, approaching the commonly applied cost-effectiveness thresholds ($100,000/QALY).</p><p><strong>Conclusions: </strong>Intrapartum universal rapid HIV screening to decrease MTCT appears cost-effective in populations with high HIV incidence in the United States.</p>","PeriodicalId":13546,"journal":{"name":"Infectious Diseases in Obstetrics and Gynecology","volume":" ","pages":"6024698"},"PeriodicalIF":0.0000,"publicationDate":"2018-03-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5872626/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious Diseases in Obstetrics and Gynecology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2018/6024698","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To determine the cost-effectiveness of universal maternal HIV screening at time of delivery to decrease mother-to-child transmission (MTCT), by comparing the cost and quality-adjusted life years (QALYs) of universal rapid HIV screening at time of delivery to two current standards of care for prenatal HIV screening in the United States.
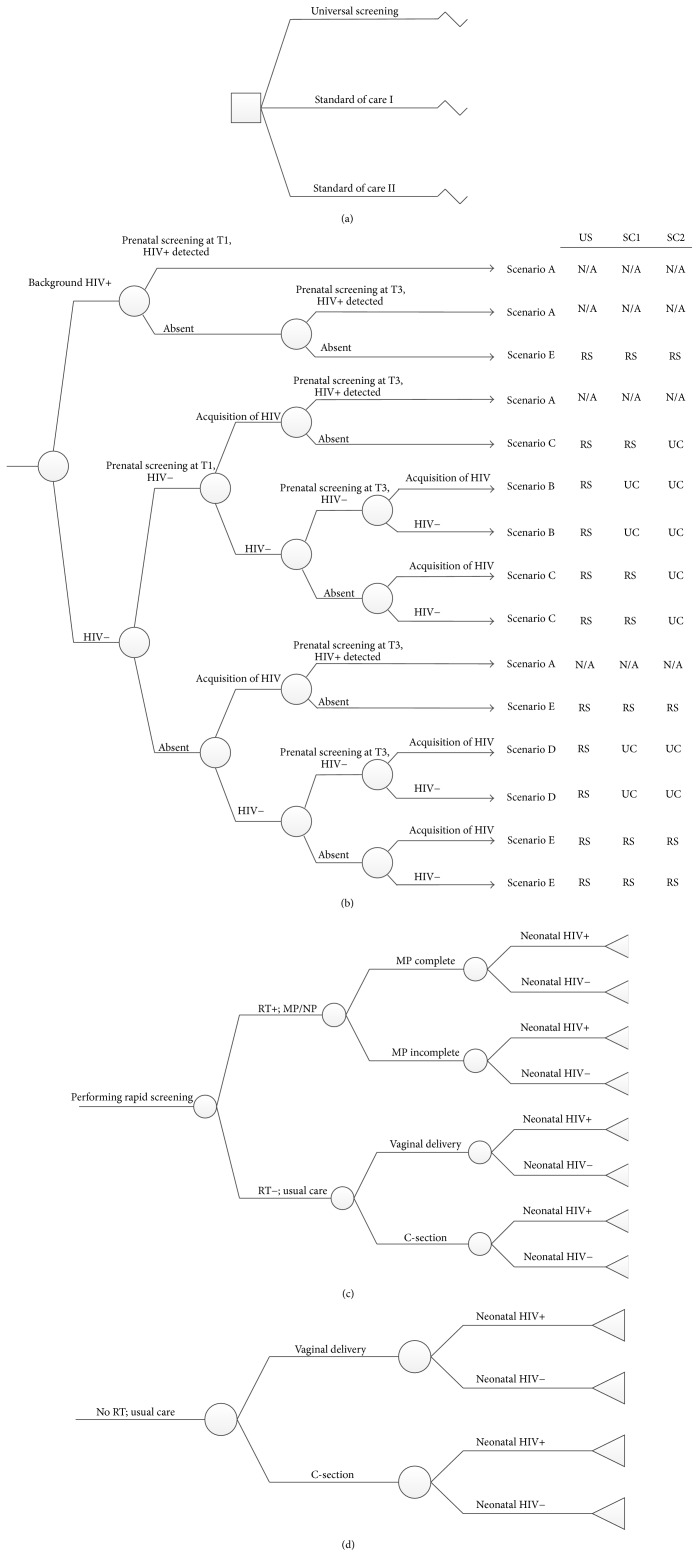
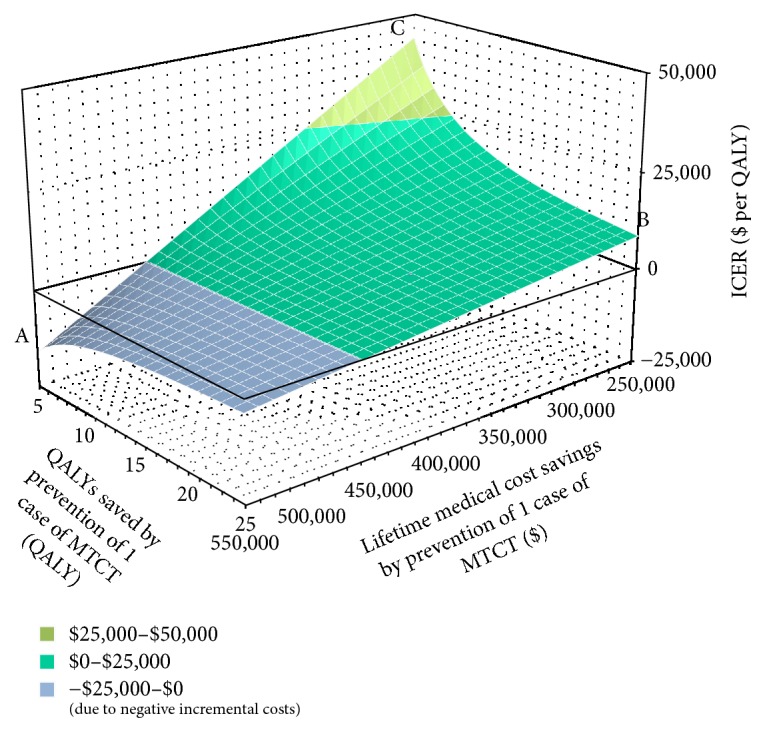
Study design: We conducted a cost-effectiveness analysis to compare the cost and QALY of universal intrapartum rapid HIV screening with two current standards of care: (I) opt-out rapid HIV testing limited to patients without previous third-trimester screening and (II) opt-out rapid HIV testing limited to patients without any prenatal screening. We developed a decision-tree model and performed sensitivity analyses to estimate the impact of variances in QALY, estimated lifetime medical costs, HIV prevalence, and cumulative incidence.
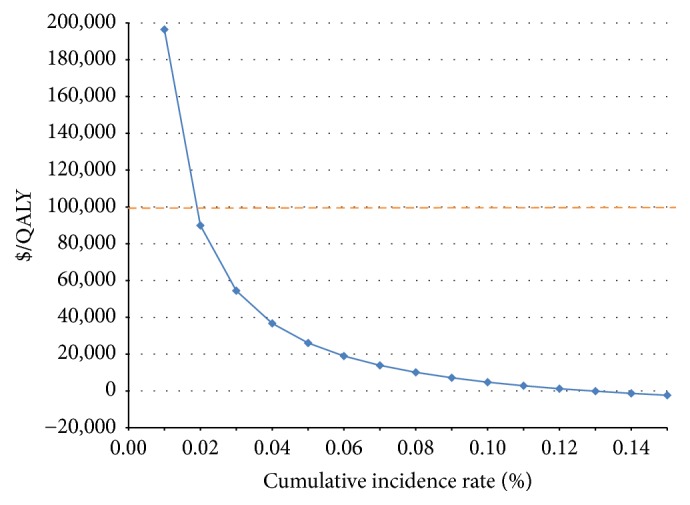
Results: The incremental cost-effectiveness ratio for universal screening was $7,973.45/QALY. The results remained robust to sensitivity analysis, except for annual cumulative incidence. In areas with an annual cumulative incidence rate of <0.02% for reproductive-age women, the incremental cost-effectiveness ratio for the expanded program would exceed $89,926.94/QALY, approaching the commonly applied cost-effectiveness thresholds ($100,000/QALY).
Conclusions: Intrapartum universal rapid HIV screening to decrease MTCT appears cost-effective in populations with high HIV incidence in the United States.
目的通过比较美国产前 HIV 筛查的两种现行标准与产时快速 HIV 筛查的成本和质量调整生命年 (QALY),确定产时普遍进行 HIV 筛查以减少母婴传播 (MTCT) 的成本效益:研究设计:我们进行了一项成本效益分析,比较了普及产时 HIV 快速筛查与两种现行医疗标准的成本和 QALY:(I) 选择不进行 HIV 快速筛查的患者仅限于未进行过第三孕期筛查的患者;(II) 选择不进行 HIV 快速筛查的患者仅限于未进行过任何产前筛查的患者。我们建立了一个决策树模型,并进行了敏感性分析,以估计 QALY、估计终生医疗成本、HIV 感染率和累积发病率等因素的影响:普遍筛查的增量成本效益比为 7,973.45 美元/QALY。除年度累计发病率外,其他结果对敏感性分析仍具有稳健性。在年累计发病率为结论:在美国 HIV 高发人群中,通过产前普及 HIV 快速筛查来减少母婴传播似乎具有成本效益。
期刊介绍:
Infectious Diseases in Obstetrics and Gynecology aims to disseminate new and important information to clinicians and other health care providers, scientists, and researchers involved in the study or treatment of infectious diseases, especially those affecting the female patient. Its ultimate aim is to advance knowledge and encourage research, thereby improving the prevention or diagnosis and treatment of patients affected by such diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


