Pyosalpinges after hysterosalpingography in a patient with lower genital tract infection and managed by laparoscopic surgery in a resource low tertiary hospital case report and literature review.
Thomas Obinchemti Egbe, Fidelia Mbi Kobenge, Metogo Mbengono Junette Arlette, Eugene Belley-Priso
{"title":"Pyosalpinges after hysterosalpingography in a patient with lower genital tract infection and managed by laparoscopic surgery in a resource low tertiary hospital case report and literature review.","authors":"Thomas Obinchemti Egbe, Fidelia Mbi Kobenge, Metogo Mbengono Junette Arlette, Eugene Belley-Priso","doi":"10.1186/s40738-018-0047-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pyosalpinges (a complication of pelvic inflammatory disease) is infection of the fallopian tubes and the morbidity associated with it has major health implications. We are reporting a case of pyosalpinges diagnosed after hysterosalpingography and managed by laparoscopic surgery at the Douala General Hospital, Cameroon.</p><p><strong>Case presentation: </strong>A 29-year-old single woman, an assistant nurse of the Douala tribe in Cameroon. She is G1P0010 and came to our attention because of secondary infertility of three years duration. She has a history consistent with four lifetime sexual partners, self-medication for chlamydia trachomatis infection and induced abortion by dilatation and aspiration. Furthermore, she is HIV positive and had an ultrasound scan suggestive of bilateral hydrosalpinges. After a hysterosalpingography examination she developed painless muco-purulent vaginal discharge and bilateral adnexal tenderness on bimanual examination suggestive of pyosalpinges. Vaginal and cervical cultures isolated Ureaplasma urealyticum and Gardnerella vaginalis sensitive to ofloxacin and metronidazole, respectively.At laparoscopy, bilateral pyosalpinges, pelvic adhesions and peri-hepatic adhesions were found. Bilateral salpingectomy with adhesiolysis including lysis of perihepatic adhesions and peritoneal toileting was done. She was discharged from hospital 72 h later and her hospital stay was uneventful. She was counseled for in-vitro fertilization and to register in the national HIV treatment programme. Her husband was prescribed ofloxacin empirically.</p><p><strong>Conclusion: </strong>Antimicrobial prophylaxis should be given to patients prior to HSG, especially those with a history of chlamydia or evidence of hydrosalpinges. There should also be universal STI testing in high risk and HIV positive patients or the danger for suboptimal antibiotic usage in areas where self-medication is common.In resource-low tertiary hospitals where computed tomography or magnetic resonance imaging is not readily available and/or affordable, clinical examination and pelvic ultrasound remains the key diagnostic tool. Surgical treatment is the best option for pyosalpinges and when plausible, laparoscopic surgery is the treatment of choice. Laparotomy is the mainstay in most hospitals in Cameroon. The parent of the patient did not consent to histo-pathologic examination.</p>","PeriodicalId":87254,"journal":{"name":"Fertility research and practice","volume":"4 ","pages":"2"},"PeriodicalIF":0.0000,"publicationDate":"2018-04-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5898046/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Fertility research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40738-018-0047-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Pyosalpinges (a complication of pelvic inflammatory disease) is infection of the fallopian tubes and the morbidity associated with it has major health implications. We are reporting a case of pyosalpinges diagnosed after hysterosalpingography and managed by laparoscopic surgery at the Douala General Hospital, Cameroon.
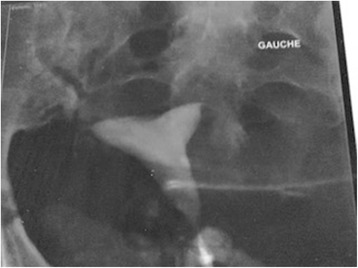
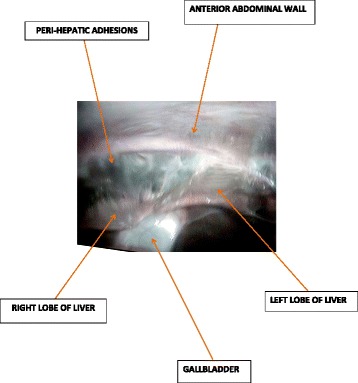
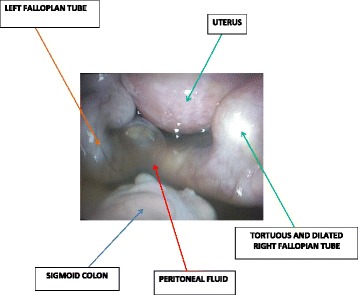
Case presentation: A 29-year-old single woman, an assistant nurse of the Douala tribe in Cameroon. She is G1P0010 and came to our attention because of secondary infertility of three years duration. She has a history consistent with four lifetime sexual partners, self-medication for chlamydia trachomatis infection and induced abortion by dilatation and aspiration. Furthermore, she is HIV positive and had an ultrasound scan suggestive of bilateral hydrosalpinges. After a hysterosalpingography examination she developed painless muco-purulent vaginal discharge and bilateral adnexal tenderness on bimanual examination suggestive of pyosalpinges. Vaginal and cervical cultures isolated Ureaplasma urealyticum and Gardnerella vaginalis sensitive to ofloxacin and metronidazole, respectively.At laparoscopy, bilateral pyosalpinges, pelvic adhesions and peri-hepatic adhesions were found. Bilateral salpingectomy with adhesiolysis including lysis of perihepatic adhesions and peritoneal toileting was done. She was discharged from hospital 72 h later and her hospital stay was uneventful. She was counseled for in-vitro fertilization and to register in the national HIV treatment programme. Her husband was prescribed ofloxacin empirically.
Conclusion: Antimicrobial prophylaxis should be given to patients prior to HSG, especially those with a history of chlamydia or evidence of hydrosalpinges. There should also be universal STI testing in high risk and HIV positive patients or the danger for suboptimal antibiotic usage in areas where self-medication is common.In resource-low tertiary hospitals where computed tomography or magnetic resonance imaging is not readily available and/or affordable, clinical examination and pelvic ultrasound remains the key diagnostic tool. Surgical treatment is the best option for pyosalpinges and when plausible, laparoscopic surgery is the treatment of choice. Laparotomy is the mainstay in most hospitals in Cameroon. The parent of the patient did not consent to histo-pathologic examination.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


