Emin Gurleyik, Fuat Cetin, Sami Dogan, Erman Yekenkurul, Ufuk Onsal, Fatih Gursoy, Alper Ipor
{"title":"Displacement of the Recurrent Laryngeal Nerve in Patients with Recurrent Goiter Undergoing Redo Thyroid Surgery.","authors":"Emin Gurleyik, Fuat Cetin, Sami Dogan, Erman Yekenkurul, Ufuk Onsal, Fatih Gursoy, Alper Ipor","doi":"10.1155/2018/4763712","DOIUrl":null,"url":null,"abstract":"<p><p>Thyroid reoperations are surgically challenging because of scarring and disturbances in the anatomy of the recurrent laryngeal nerve (RLN). This study was conducted on 49 patients who underwent redo surgery. 61 RLNs were identified and completely exposed. Their functional integrity was evaluated using intraoperative nerve monitoring (IONM). Indications for secondary surgery, anatomical changes secondary to recurrent goiter mass and prior surgery, and results of IONM were studied. Frequent indications for redo surgery were multinodular goiter (MNG) in 19 (38.8%) and results of cytology in 14 (28.5%) patients. The mean time interval between primary and redo thyroid surgery was 23.4 years. We laterally approached 41 (67.2%) thyroid lobes between the sternocleidomastoid and sternohyoid muscles. 16 (26.2%) RLNs were found to be adherent to the lateral surface of the corresponding thyroid lobe. The functional integrity of all RLNs was confirmed by IONM. The remnant thyroid tissue can then lead to goiter recurrence requiring secondary surgery after a long period of time. The indications for redo surgery were similar to primary cases. Lateral displacement of the RLN which is adherent to the lateral surface of recurrent goiter mass is common anatomic variation. Thyroid reoperations based on awareness of anatomical disturbances can be performed safely by an experienced surgeon with support of ancillary electrophysiological technology.</p>","PeriodicalId":17394,"journal":{"name":"Journal of Thyroid Research","volume":"2018 ","pages":"4763712"},"PeriodicalIF":1.7000,"publicationDate":"2018-02-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2018/4763712","citationCount":"7","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Thyroid Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2018/4763712","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 7
Abstract
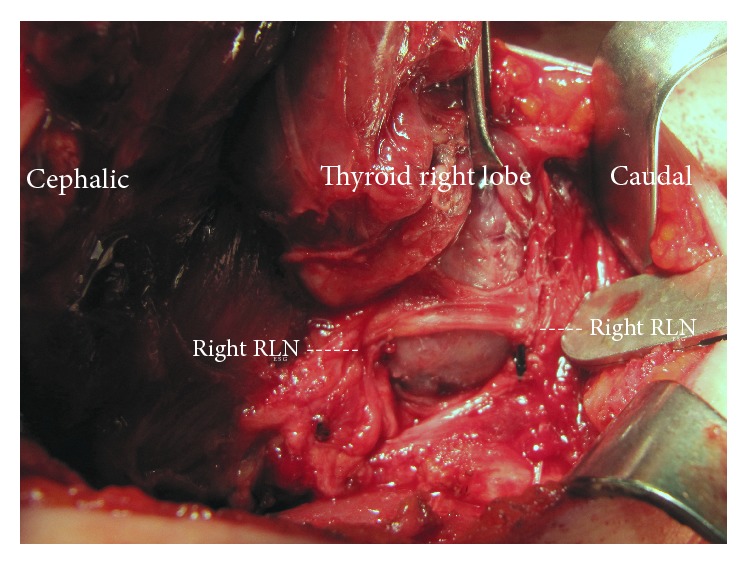
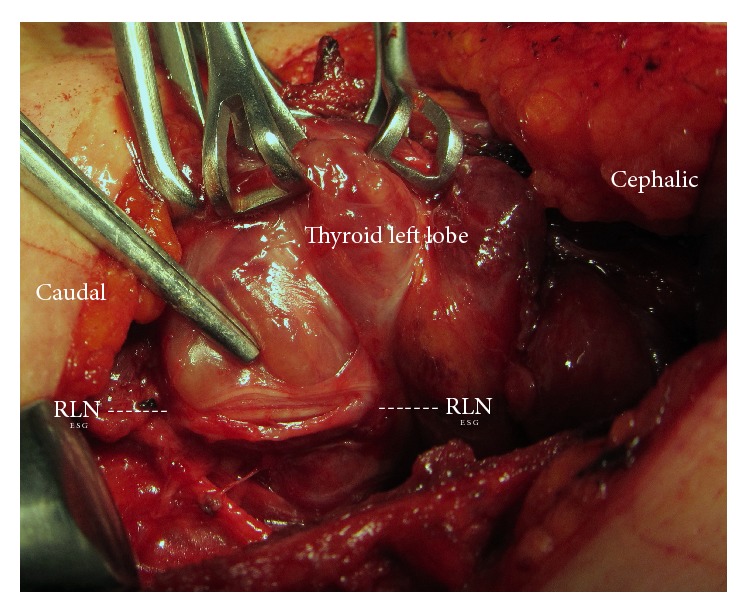
Thyroid reoperations are surgically challenging because of scarring and disturbances in the anatomy of the recurrent laryngeal nerve (RLN). This study was conducted on 49 patients who underwent redo surgery. 61 RLNs were identified and completely exposed. Their functional integrity was evaluated using intraoperative nerve monitoring (IONM). Indications for secondary surgery, anatomical changes secondary to recurrent goiter mass and prior surgery, and results of IONM were studied. Frequent indications for redo surgery were multinodular goiter (MNG) in 19 (38.8%) and results of cytology in 14 (28.5%) patients. The mean time interval between primary and redo thyroid surgery was 23.4 years. We laterally approached 41 (67.2%) thyroid lobes between the sternocleidomastoid and sternohyoid muscles. 16 (26.2%) RLNs were found to be adherent to the lateral surface of the corresponding thyroid lobe. The functional integrity of all RLNs was confirmed by IONM. The remnant thyroid tissue can then lead to goiter recurrence requiring secondary surgery after a long period of time. The indications for redo surgery were similar to primary cases. Lateral displacement of the RLN which is adherent to the lateral surface of recurrent goiter mass is common anatomic variation. Thyroid reoperations based on awareness of anatomical disturbances can be performed safely by an experienced surgeon with support of ancillary electrophysiological technology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


