Samuel C Ohaegbulam, Wilfred C Mezue, Chika Anele Ndubuisi, Mark O Chikani, Ndubuisi D Achebe, Uwadiegwu A Erechukwu
{"title":"Modified Laminoplasty for Degenerative Cervical Spondylosis: The Technique of Floating Laminoplasty.","authors":"Samuel C Ohaegbulam, Wilfred C Mezue, Chika Anele Ndubuisi, Mark O Chikani, Ndubuisi D Achebe, Uwadiegwu A Erechukwu","doi":"10.4103/njs.NJS_12_17","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Laminoplasty is an established alternative to laminectomy for posterior cervical decompression in spondylotic myelopathy. However, standard laminoplasty requires internal fixation, which is often not obtainable in developing countries. We present our experience with a technique of noninstrumented (floating) laminoplasty developed to avoid the need to anchor the laminoplasty to the anterior elements.</p><p><strong>Methods: </strong>We have used floating laminoplasty (FL) for posterior cervical decompression in patients with cervical spondylosis since 2004 and report the technique and our experience with it between 2009 and 2014 when C-arm and magnetic resonance imaging became available in our unit. Patients who had classical laminectomy and hemilaminectomies were excluded. The operation involved bilateral approach to the laminae through a midline incision with generous sparing of the supraspinous, interspinal and interlaminar ligaments. During closure the laminoplasty was hitched to the ligamentum nuchae. Nurick grading was used for clinical evaluation. Patients were followed for at least 1 year.</p><p><strong>Results: </strong>There were 36 patients with age range between 32 and 72 years (mean: 56.5 years). Male to female ratio was 3:1. Most patients presented with advanced disease, with 25%, 36%, and 30% at Nurick Grade 3, 4, and 5, respectively. Postoperatively, all (100%) patients with Nurick Grade 2 and 3 improved to Grade 1 or 0, while 9 (69%) of the 13 at Grade 4 improved to Grade 2 or better. Only 1 (9.1%) of 11 operated at Grade 5 did not improve while 3 (27%) improved to Grade 2 or better. No postoperative instability was identified on follow-up.</p><p><strong>Conclusion: </strong>FL is a safe and simple procedure that preserves spine stability and minimizes postoperative spinal deformity.</p>","PeriodicalId":30399,"journal":{"name":"Nigerian Journal of Surgery","volume":"24 1","pages":"1-5"},"PeriodicalIF":0.0000,"publicationDate":"2018-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f1/12/NJS-24-1.PMC5883842.pdf","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nigerian Journal of Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/njs.NJS_12_17","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 4
Abstract
Background: Laminoplasty is an established alternative to laminectomy for posterior cervical decompression in spondylotic myelopathy. However, standard laminoplasty requires internal fixation, which is often not obtainable in developing countries. We present our experience with a technique of noninstrumented (floating) laminoplasty developed to avoid the need to anchor the laminoplasty to the anterior elements.
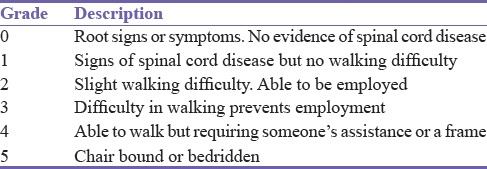
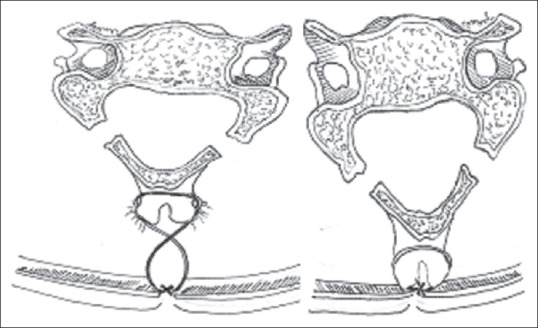
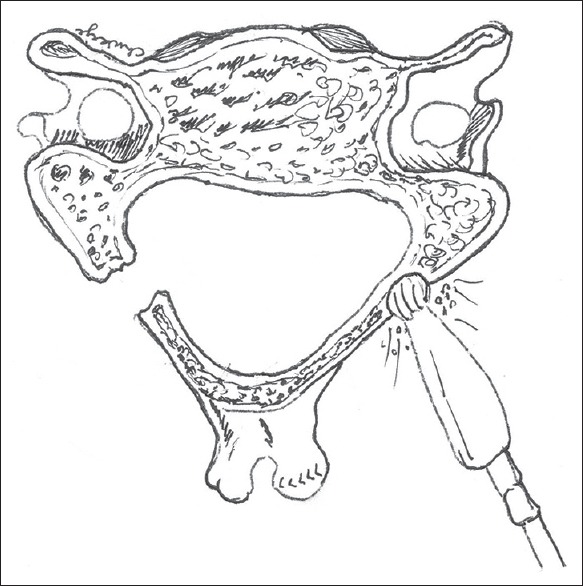
Methods: We have used floating laminoplasty (FL) for posterior cervical decompression in patients with cervical spondylosis since 2004 and report the technique and our experience with it between 2009 and 2014 when C-arm and magnetic resonance imaging became available in our unit. Patients who had classical laminectomy and hemilaminectomies were excluded. The operation involved bilateral approach to the laminae through a midline incision with generous sparing of the supraspinous, interspinal and interlaminar ligaments. During closure the laminoplasty was hitched to the ligamentum nuchae. Nurick grading was used for clinical evaluation. Patients were followed for at least 1 year.
Results: There were 36 patients with age range between 32 and 72 years (mean: 56.5 years). Male to female ratio was 3:1. Most patients presented with advanced disease, with 25%, 36%, and 30% at Nurick Grade 3, 4, and 5, respectively. Postoperatively, all (100%) patients with Nurick Grade 2 and 3 improved to Grade 1 or 0, while 9 (69%) of the 13 at Grade 4 improved to Grade 2 or better. Only 1 (9.1%) of 11 operated at Grade 5 did not improve while 3 (27%) improved to Grade 2 or better. No postoperative instability was identified on follow-up.
Conclusion: FL is a safe and simple procedure that preserves spine stability and minimizes postoperative spinal deformity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


