Rony-Orijit Dey Hazra, Helmut Lill, Gunnar Jensen, Julia Imrecke, Alexander Ellwein
{"title":"Fracture-pattern-related therapy concepts in distal humeral fractures.","authors":"Rony-Orijit Dey Hazra, Helmut Lill, Gunnar Jensen, Julia Imrecke, Alexander Ellwein","doi":"10.1007/s11678-018-0442-8","DOIUrl":null,"url":null,"abstract":"<p><p>Around one third of humeral fractures and 2-6% of all fractures occur to the distal part of the humerus. There is a bimodal distribution differentiating between young male patients with high-energy and elderly female patients with low-energy trauma related to osteoporosis. The AO classification and Dubberley subclassification are used in daily routine. Most fractures are diagnosed on radiographs. For further evaluation, three-dimensional computed tomography is recommended, especially for comminuted or complex fractures. Owing to the long immobilization and resultant poor functional outcome, conservative treatment is followed for inoperable patients. The operative approach and osteosynthesis depend on the fracture pattern. In A1 avulsion fractures, open reduction and screw fixation are recommended. In A2/A3 fractures, a triceps-sparing approach following a 90° double-plate construction (radial dorsal/ulnar lateral) with locking plates is favored. Partial articular B1/B2 fractures are exposed via a medial or lateral approach using unilateral locking plates to stabilize the medial/lateral column. Coronal shear fractures (B3) are classified after Dubberley and are treated via an extended Kocher approach and headless compression screws in anteroposterior direction. If there is a further posterior comminution or a lateral column fragment, stabilization is needed for the lateral/medial column with a precontoured locking plate. In solely articular fracture patterns, a dorsal approach with either a 90° or 180° double-plate construction is advised. If a reconstruction is not possible owing to fracture complexity or bone quality, total elbow arthroplasty is a viable option. However, lifelong limitation in weight-bearing up to 5 kg, limited longevity, and the potential for complicated revision surgery should be considered.</p>","PeriodicalId":43682,"journal":{"name":"Obere Extremitaet-Schulter-Ellenbogen-Hand-Upper Extremity-Shoulder Elbow Hand","volume":"13 1","pages":"23-32"},"PeriodicalIF":0.3000,"publicationDate":"2018-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1007/s11678-018-0442-8","citationCount":"16","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Obere Extremitaet-Schulter-Ellenbogen-Hand-Upper Extremity-Shoulder Elbow Hand","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s11678-018-0442-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/2/15 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 16
Abstract
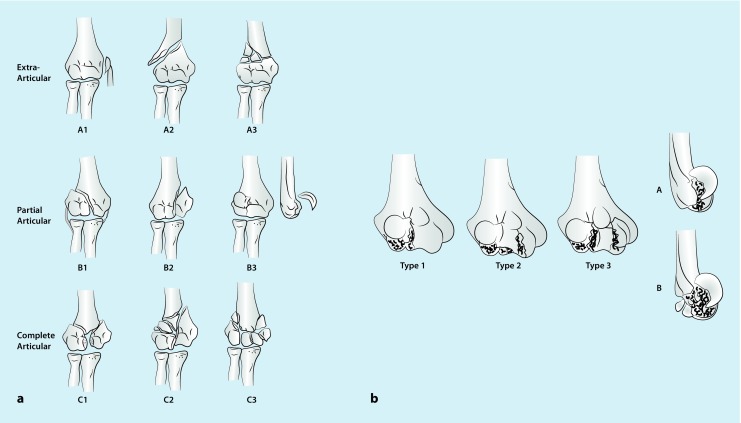
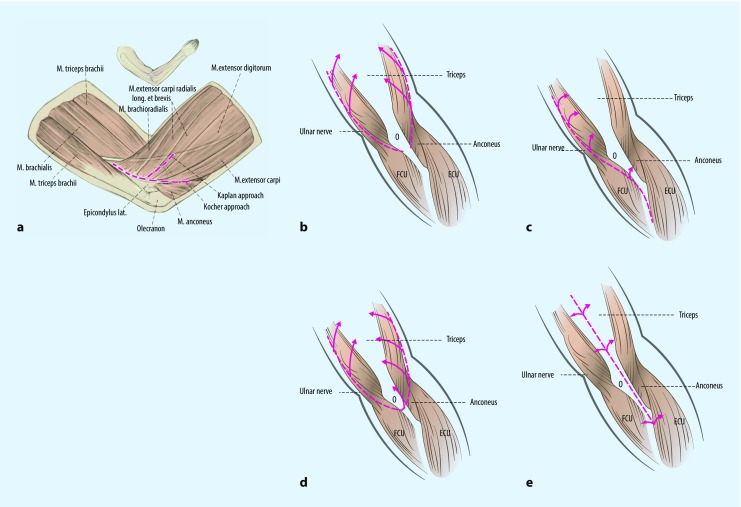
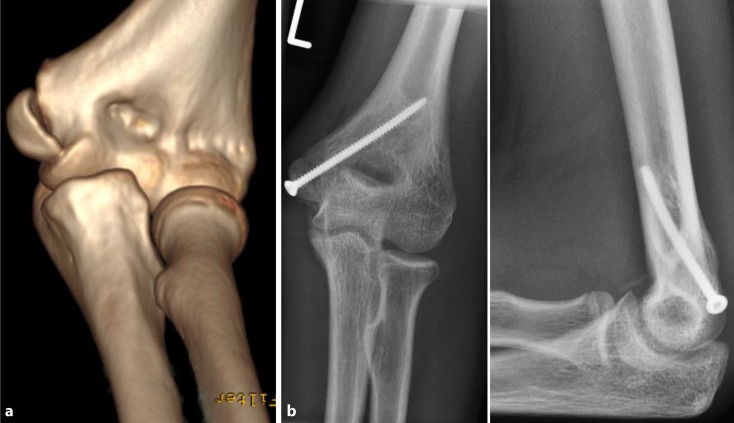
Around one third of humeral fractures and 2-6% of all fractures occur to the distal part of the humerus. There is a bimodal distribution differentiating between young male patients with high-energy and elderly female patients with low-energy trauma related to osteoporosis. The AO classification and Dubberley subclassification are used in daily routine. Most fractures are diagnosed on radiographs. For further evaluation, three-dimensional computed tomography is recommended, especially for comminuted or complex fractures. Owing to the long immobilization and resultant poor functional outcome, conservative treatment is followed for inoperable patients. The operative approach and osteosynthesis depend on the fracture pattern. In A1 avulsion fractures, open reduction and screw fixation are recommended. In A2/A3 fractures, a triceps-sparing approach following a 90° double-plate construction (radial dorsal/ulnar lateral) with locking plates is favored. Partial articular B1/B2 fractures are exposed via a medial or lateral approach using unilateral locking plates to stabilize the medial/lateral column. Coronal shear fractures (B3) are classified after Dubberley and are treated via an extended Kocher approach and headless compression screws in anteroposterior direction. If there is a further posterior comminution or a lateral column fragment, stabilization is needed for the lateral/medial column with a precontoured locking plate. In solely articular fracture patterns, a dorsal approach with either a 90° or 180° double-plate construction is advised. If a reconstruction is not possible owing to fracture complexity or bone quality, total elbow arthroplasty is a viable option. However, lifelong limitation in weight-bearing up to 5 kg, limited longevity, and the potential for complicated revision surgery should be considered.
期刊介绍:
Zielsetzung der Zeitschrift
Die Zeitschrift Obere Extremität widmet sich der Versorgung von Verletzungen, Verletzungsfolgen und Erkrankungen im Bereich des Schulter- und des Ellenbogengelenks.
Frei eingereichte Originalien präsentieren Forschungsergebnisse aktueller Studien im Bereich der Schulter- und Ellenbogenchirurgie und fördern den wissenschaftlichen Austausch. Vielversprechende Studien, die derzeit durchgeführt werden, sind ebenso willkommen, wie Langzeitstudien, die bewährte Verfahren auf den Prüfstand stellen. Fallberichte beleuchten seltene Indikationen und schildern ungewöhnliche Behandlungsverläufe.
Umfassende Übersichtsarbeiten zu einem aktuellen Schwerpunktthema sind das Kernstück jeder Ausgabe. Im Mittelpunkt steht gesichertes Wissen mit hoher Relevanz für die tägliche Arbeit in der Schulter- und Ellenbogenchirurgie. Zusätzlich wird in speziellen Rubriken über innovative Behandlungsmaßnahmen, Probleme in der Begutachtung, berufspolitische Entwicklungen und Kongressaktivitäten berichtet.
Als gemeinsames Kommunikations- und Weiterbildungsforum für alle Chirurg*innen und Orthopäd*innen mit entsprechender Spezialisierung ist die Zeitschrift Obere Extremität zukunftsorientiert und schließt eine wichtige Lücke im orthopädisch-unfallchirurgischen Informationsangebot.
Aims & scope
The journal Obere Extremität (Upper Extremity) is dedicated to the treatment of injuries, consequences of injuries and diseases in the area of the shoulder and elbow joint.
Freely submitted originals present research results of current studies in the field of shoulder and elbow surgery and promote scientific exchange. Promising studies that are currently being carried out are welcome, as are long-term studies that put proven procedures to the test. Case reports illuminate rare indications and describe unusual courses of treatment.
Comprehensive reviews on a current focus topic are the core of each issue. The focus is on secured knowledge with high relevance for the daily work in shoulder and elbow surgery. In addition, special sections report on innovative treatment measures, problems in assessment, professional policy developments and congress activities.
As a joint communication and further education forum for all surgeons and orthopaedic surgeons with appropriate specialisation, the journal Obere Extremität is future-oriented and closes an important gap in the orthopaedic trauma surgery information offer.
Begutachtung / Peer Review
Alle Beiträge, die bei der Zeitschrift Obere Extremität eingereicht werden (einschließlich der eingeladenen Manuskripte) durchlaufen ein Doppelblind-Peer-Review-Verfahren, an dem mindestens zwei unabhängige Experten beteiligt sind.---
All manuscripts submitted to the journal Obere Extremität (including invited manuscripts) undergo a double-blind peer review process involving at least two independent experts.
Ethische Richtlinien / Best Practice Guidelines and Publication Ethics
Die Zeitschrift Obere Extremität folgt den Richtlinien des Komitees für Publikationsethik (COPE). Autoren wird empfohlen, klinische Studien, die sie zur Veröffentlichung in Betracht ziehen, vor der Veröffentlichung in kostenlosen, öffentlichen Registern für klinische Studien (z.B. www.clinicaltrials.gov, http://clinicaltrials.ifpma.org, http://isrctn.org, www.germanctr.de/online-Register_de.html) zu registrieren. Die Register sind nach den Richtlinien des International Committee of Medical Journal Editors (ICMJE) zu genehmigen. Die Autor*innen sollten am Ende ihres Abstracts den Namen des Studienregisters und ihre Registriernummer für klinische Studien angeben.
The journal Obere Extremität (Upper Extremity) follows the Committee of Publications Ethics (COPE) - Guidelines. Authors are recommended to register clinical trials they consider for publication in free, public clinical trial registries (e.g., www.clinicaltrials.gov, http://clinicaltrials.ifpma.org, http://isrctn.org, www.germanctr.de/online-Register_de.html) before publication. The registries are to be approved by the guidelines of the International Committee of Medical Journal Editors (ICMJE). Authors should include the name of the trial register and their clinical trial registration number at the end of their abstract.
Deklaration von Helsinki / Declaration of Helsinki
Alle zur Veröffentlichung eingereichten Manuskripte, die Ergebnisse von Studien an Proband*innen oder Patient*innen präsentieren, müssen gemäß den Autorenrichtlinien für Originalarbeiten der Deklaration von Helsinki entsprechen.
All Manuscripts submitted for publication presenting results from studies on probands or patients must comply with the Declaration of Helsinki according to the author guidelines for original papers.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


