Antonio Maria Calafiore , Angela Lorena Iacò , Daniela Clemente , Reda Refaie , Silvio Romano , Mahmood Asif , Maria Penco , Michele Di Mauro
{"title":"Repair or prosthesis insertion in ischemic mitral regurgitation: Two faces of the same medal","authors":"Antonio Maria Calafiore , Angela Lorena Iacò , Daniela Clemente , Reda Refaie , Silvio Romano , Mahmood Asif , Maria Penco , Michele Di Mauro","doi":"10.1016/j.ijchv.2014.02.002","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><p>The proper treatment of chronic ischemic mitral regurgitation (CIMR) is still under evaluation. The different role of mitral valve repair (MVr) or mitral valve prosthesis insertion (MVPI) is still not defined.</p></div><div><h3>Methods</h3><p>From May 2009 to December 2011 167 patients with ejection fraction (EF) ≤ 40% had MV surgery for CIMR, MVr in 135 (80.8%) and MVPI in 32 (19.2%). Indication to MVPI was a MV coaptation depth > 10 mm. EF was lower (26 ± 7 vs 32 ± 6, p = 0.0000) in MVPI, whereas MR grade (3.6 ± 0.8 vs 2.7 ± 0.9, p = 0.0000), left ventricle dimensions (end diastolic, LVEDD, 62 ± 7 vs 57 ± 6 mm, p = 0.0001; end systolic, LVESD, 49 ± 8 vs 44 ± 8 mm, p = 0.0018), systolic pulmonary artery pressure (51 ± 22 vs 41 ± 16 mm Hg, p = 0.0037) and NYHA Class (3.6 ± 0.5 vs 2.8 ± 0.6, p = 0.0000) were higher.</p></div><div><h3>Results</h3><p>In-hospital mortality was similar (3.1 vs 3.7%) as well as 3-year survival (86 ± 6 vs 88 ± 4) and survival in NYHA Class I/II (80 ± 5 vs 83 ± 4). One hundred thirty nine patients had an echocardiographic evaluation after a minimum of 4 months (13 ± 8). EF rose significantly in both groups (from 26 ± 7% to 30 ± 4%, p = 0.0122, and from 32 ± 6% to 35 ± 8%, p = 0.0018). LVESD reduced significantly in both groups (from 49 ± 8 to 43 ± 9 mm, p = 0.0109, and from 44 ± 8 to 41 ± 7 mm, p = 0.0033). MR grade was significantly lower in patients who had MVPI (0.1 ± 0.2 vs 0.3 ± 0.3, p = 0.0011).</p></div><div><h3>Conclusions</h3><p>With appropriate indications, MVPI is a safe procedure which provides similar results to MVr with lower MR return, even if addressed to patients with worse preoperative parameters.</p></div>","PeriodicalId":90542,"journal":{"name":"International journal of cardiology. Heart & vessels","volume":"3 ","pages":"Pages 32-36"},"PeriodicalIF":0.0000,"publicationDate":"2014-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1016/j.ijchv.2014.02.002","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International journal of cardiology. Heart & vessels","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2214763214000054","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
Abstract
Objective
The proper treatment of chronic ischemic mitral regurgitation (CIMR) is still under evaluation. The different role of mitral valve repair (MVr) or mitral valve prosthesis insertion (MVPI) is still not defined.
Methods
From May 2009 to December 2011 167 patients with ejection fraction (EF) ≤ 40% had MV surgery for CIMR, MVr in 135 (80.8%) and MVPI in 32 (19.2%). Indication to MVPI was a MV coaptation depth > 10 mm. EF was lower (26 ± 7 vs 32 ± 6, p = 0.0000) in MVPI, whereas MR grade (3.6 ± 0.8 vs 2.7 ± 0.9, p = 0.0000), left ventricle dimensions (end diastolic, LVEDD, 62 ± 7 vs 57 ± 6 mm, p = 0.0001; end systolic, LVESD, 49 ± 8 vs 44 ± 8 mm, p = 0.0018), systolic pulmonary artery pressure (51 ± 22 vs 41 ± 16 mm Hg, p = 0.0037) and NYHA Class (3.6 ± 0.5 vs 2.8 ± 0.6, p = 0.0000) were higher.
Results
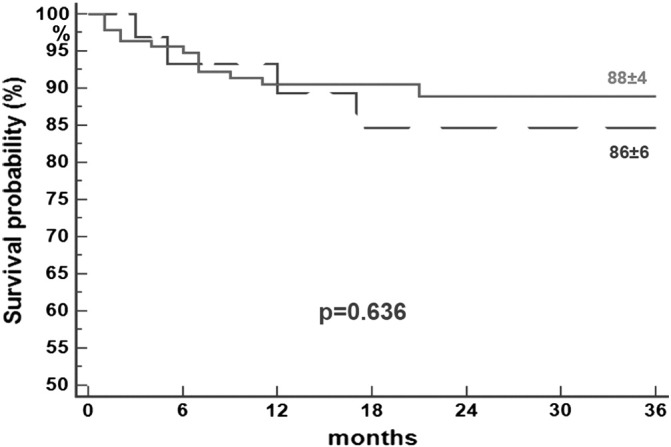
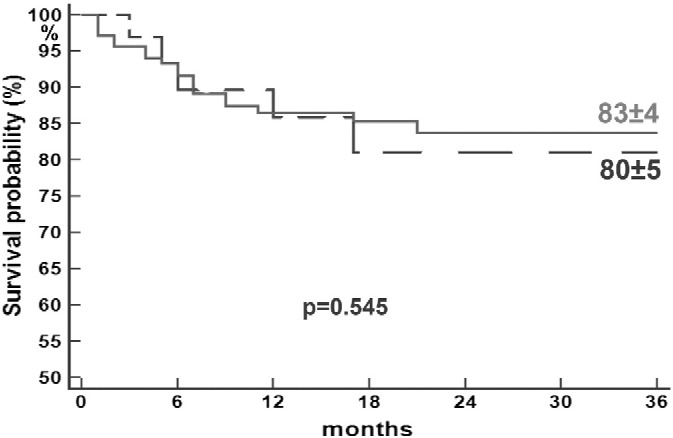
In-hospital mortality was similar (3.1 vs 3.7%) as well as 3-year survival (86 ± 6 vs 88 ± 4) and survival in NYHA Class I/II (80 ± 5 vs 83 ± 4). One hundred thirty nine patients had an echocardiographic evaluation after a minimum of 4 months (13 ± 8). EF rose significantly in both groups (from 26 ± 7% to 30 ± 4%, p = 0.0122, and from 32 ± 6% to 35 ± 8%, p = 0.0018). LVESD reduced significantly in both groups (from 49 ± 8 to 43 ± 9 mm, p = 0.0109, and from 44 ± 8 to 41 ± 7 mm, p = 0.0033). MR grade was significantly lower in patients who had MVPI (0.1 ± 0.2 vs 0.3 ± 0.3, p = 0.0011).
Conclusions
With appropriate indications, MVPI is a safe procedure which provides similar results to MVr with lower MR return, even if addressed to patients with worse preoperative parameters.
目的探讨慢性缺血性二尖瓣反流(CIMR)的正确治疗方法。二尖瓣修复(MVr)或二尖瓣假体插入(MVPI)的不同作用仍未明确。方法2009年5月~ 2011年12月167例射血分数(EF)≤40%的患者因CIMR行MV手术,其中MVr 135例(80.8%),MVPI 32例(19.2%)。MVPI的指示是MV适配深度>10毫米。MVPI患者EF较低(26±7 vs 32±6,p = 0.0000),而MR分级(3.6±0.8 vs 2.7±0.9,p = 0.0000),左心室尺寸(舒张末期,LVEDD, 62±7 vs 57±6 mm, p = 0.0001;收缩期末期,LVESD, 49±8 vs 44±8 mm, p = 0.0018),收缩期肺动脉压(51±22 vs 41±16 mm Hg, p = 0.0037)和NYHA分级(3.6±0.5 vs 2.8±0.6,p = 0.0000)较高。ResultsIn-hospital死亡率相似(3.7% vs 3.1)以及3年存活率(86±6 vs 88±4)和生存NYHA班上I / II(80±5 vs 83±4)。一百三十九例患者有至少4个月后超声心动图评价(13±8)。两组EF显著上升(从26到30±7%±4%,p = 0.0122,从32到35±6%±8%,p = 0.0018)。两组LVESD均显著减少(从49±8到43±9 mm, p = 0.0109,从44±8到41±7 mm, p = 0.0033)。MVPI患者的MR分级明显较低(0.1±0.2 vs 0.3±0.3,p = 0.0011)。结论:在适当的适应症下,MVPI是一种安全的手术,即使针对术前参数较差的患者,也能提供与MVr相似的结果,但MR回报率较低。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


