S W Olson, J J Lee, M Poirier, D J Little, L K Prince, T P Baker, J D Edison, K C Abbott
{"title":"Anti-Myeloperoxidase Antibodies Associate with Future Proliferative Lupus Nephritis.","authors":"S W Olson, J J Lee, M Poirier, D J Little, L K Prince, T P Baker, J D Edison, K C Abbott","doi":"10.1155/2017/1872846","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The subclinical pathophysiology of proliferative lupus nephritis (PLN) has not been fully elucidated. Myeloperoxidase anti-neutrophil cytoplasmic antibody (MPO-ANCA) is associated with PLN, but prediagnostic levels have not been reported.</p><p><strong>Methods: </strong>We performed a retrospective case-control Department of Defense Serum Repository (DoDSR) study comparing MPO-ANCA levels in longitudinal prediagnostic serum samples for 23 biopsy confirmed proliferative lupus nephritis (PLN) patients to DoDSR identified age, sex, race, and age of serum matched healthy and SLE without LN disease controls. We also compared the temporal relationship of MPO-ANCA to anti-double stranded DNA antibodies (dsDNAab).</p><p><strong>Results: </strong>A greater proportion of PLN patients had prediagnostic MPO-ANCA levels above ≥3 U/mL and ≥6 U/mL compared to SLE without LN (91% versus 43%, <i>p</i> < 0.001; 57% versus 5%, <i>p</i> < 0.001, resp.). In subgroup analysis, the MPO-ANCA threshold of ≥3 U/mL was significant at <1 year (88% versus 39%, <i>p</i> = 0.007) and 1-4 years (87% versus 38%, <i>p</i> = 0.009) prior to diagnosis. Statistically significant subclinical MPO-ANCA levels (≥3 U/mL) occurred prior to statistically significant dsDNAab ≥ 3 IU/ml (89% versus 11%, <i>p</i> = 0.003).</p><p><strong>Conclusions: </strong>Subclinical MPO-ANCA levels could distinguish future PLN from SLE without LN. MPO-ANCA manifests prior to clinical disease and subclinical dsDNAab to suggest that it may contribute directly to PLN pathogenicity.</p>","PeriodicalId":46314,"journal":{"name":"Autoimmune Diseases","volume":"2017 ","pages":"1872846"},"PeriodicalIF":1.7000,"publicationDate":"2017-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2017/1872846","citationCount":"9","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Autoimmune Diseases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2017/1872846","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/12/24 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 9
Abstract
Background: The subclinical pathophysiology of proliferative lupus nephritis (PLN) has not been fully elucidated. Myeloperoxidase anti-neutrophil cytoplasmic antibody (MPO-ANCA) is associated with PLN, but prediagnostic levels have not been reported.
Methods: We performed a retrospective case-control Department of Defense Serum Repository (DoDSR) study comparing MPO-ANCA levels in longitudinal prediagnostic serum samples for 23 biopsy confirmed proliferative lupus nephritis (PLN) patients to DoDSR identified age, sex, race, and age of serum matched healthy and SLE without LN disease controls. We also compared the temporal relationship of MPO-ANCA to anti-double stranded DNA antibodies (dsDNAab).
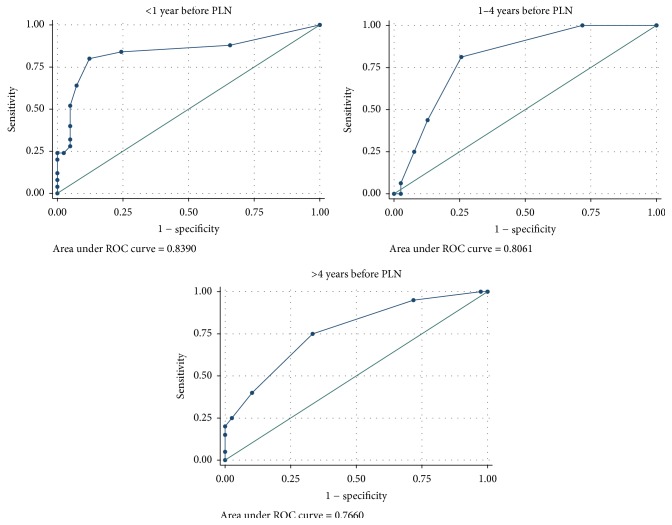
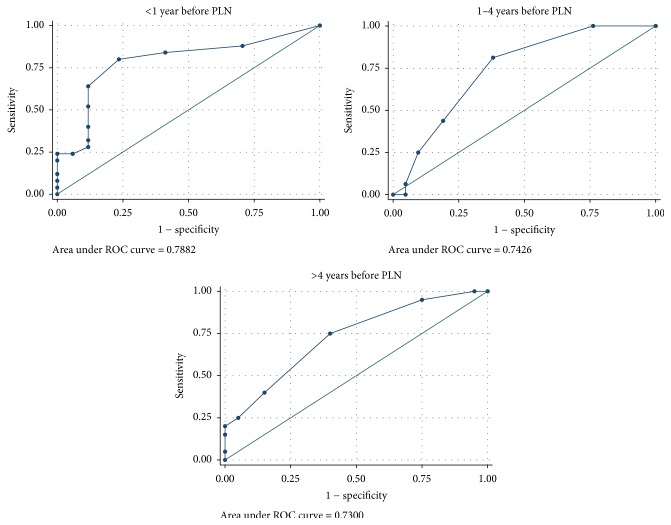
Results: A greater proportion of PLN patients had prediagnostic MPO-ANCA levels above ≥3 U/mL and ≥6 U/mL compared to SLE without LN (91% versus 43%, p < 0.001; 57% versus 5%, p < 0.001, resp.). In subgroup analysis, the MPO-ANCA threshold of ≥3 U/mL was significant at <1 year (88% versus 39%, p = 0.007) and 1-4 years (87% versus 38%, p = 0.009) prior to diagnosis. Statistically significant subclinical MPO-ANCA levels (≥3 U/mL) occurred prior to statistically significant dsDNAab ≥ 3 IU/ml (89% versus 11%, p = 0.003).
Conclusions: Subclinical MPO-ANCA levels could distinguish future PLN from SLE without LN. MPO-ANCA manifests prior to clinical disease and subclinical dsDNAab to suggest that it may contribute directly to PLN pathogenicity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


