Shin Han Song, Gyeong Ah Sim, Seon Ha Baek, Jang Won Seo, Jung Weon Shim, Ja Ryong Koo
{"title":"Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) Associated with Mediastinal Schwannoma.","authors":"Shin Han Song, Gyeong Ah Sim, Seon Ha Baek, Jang Won Seo, Jung Weon Shim, Ja Ryong Koo","doi":"10.5049/EBP.2017.15.2.42","DOIUrl":null,"url":null,"abstract":"<p><p>Syndrome of inappropriate antidiuretic hormone secretion (SIADH) is the most common cause of euvolemic hypo-osmotic hyponatremia. There are several etiologies of SIADH including neuroendocrine tumor, pulmonary disease, infection, trauma, and medications. Here, we report a case of SIADH associated with a schwannoma involving the mediastinum in a 75-year-old woman who presented with nausea, vomiting, and general weakness. Laboratory testing showed hypo-osmolar hyponatremia, with a serum sodium level of 102mmol/L, serum osmolality of 221mOsm/kg, urine osmolality of 382mOsm/kg, urine sodium of 55 mmol/L, and plasma antidiuretic hormone (ADH) of 4.40 pg/mL. Chest computed tomography identified a 1.5-cm-sized solid enhancing nodule in the right lower paratracheal area. A biopsy specimen was obtained by video-assisted thoracoscopic surgery, which was diagnosed on pathology as a schwannoma. The hyponatremia was completely resolved after schwannoma resection and plasma ADH level decreased from 4.40 pg/mL to 0.86 pg/mL. This case highlights the importance of suspecting and identifying the underlying cause of SIADH when faced with refractory or recurrent hyponatremia, and that on possibility is mediastinal schwannoma.</p>","PeriodicalId":35352,"journal":{"name":"Electrolyte and Blood Pressure","volume":"15 2","pages":"42-46"},"PeriodicalIF":0.0000,"publicationDate":"2017-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.5049/EBP.2017.15.2.42","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Electrolyte and Blood Pressure","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5049/EBP.2017.15.2.42","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/12/31 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 4
Abstract
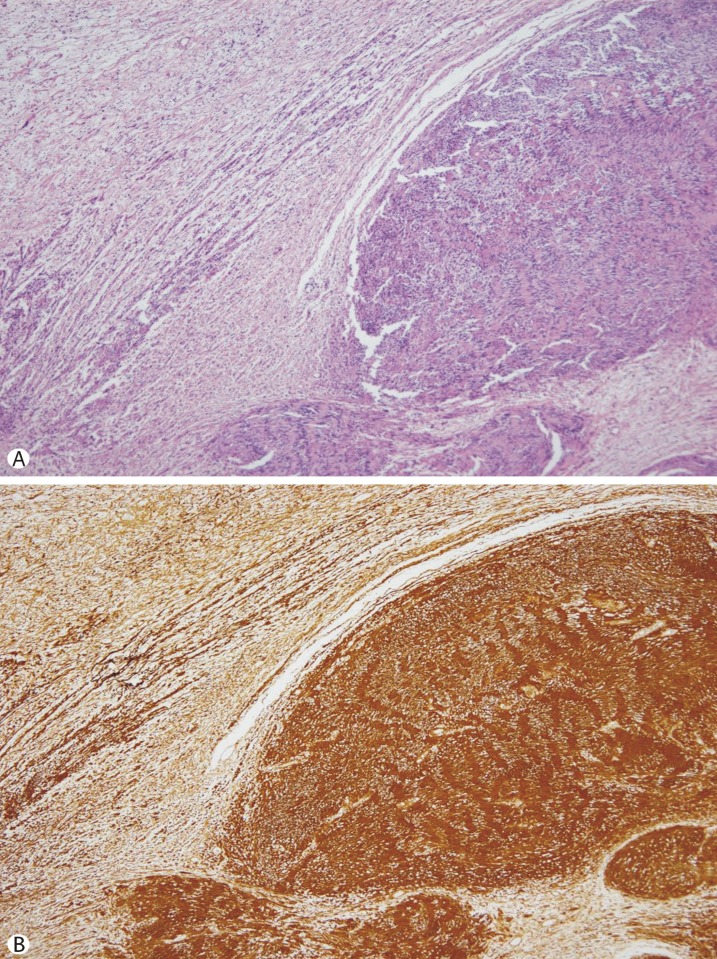
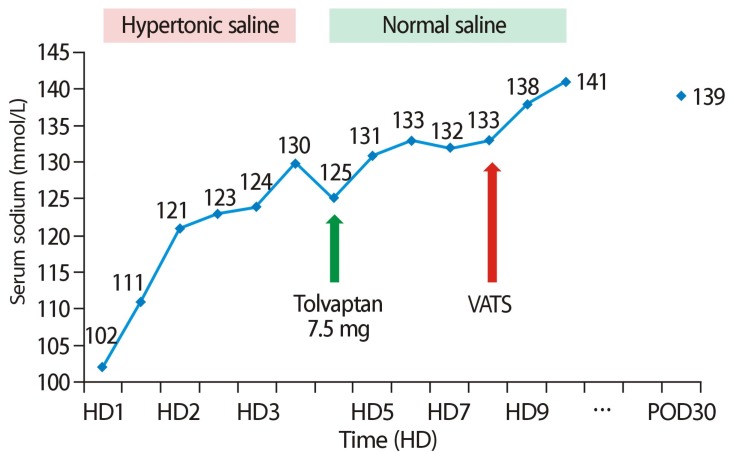
Syndrome of inappropriate antidiuretic hormone secretion (SIADH) is the most common cause of euvolemic hypo-osmotic hyponatremia. There are several etiologies of SIADH including neuroendocrine tumor, pulmonary disease, infection, trauma, and medications. Here, we report a case of SIADH associated with a schwannoma involving the mediastinum in a 75-year-old woman who presented with nausea, vomiting, and general weakness. Laboratory testing showed hypo-osmolar hyponatremia, with a serum sodium level of 102mmol/L, serum osmolality of 221mOsm/kg, urine osmolality of 382mOsm/kg, urine sodium of 55 mmol/L, and plasma antidiuretic hormone (ADH) of 4.40 pg/mL. Chest computed tomography identified a 1.5-cm-sized solid enhancing nodule in the right lower paratracheal area. A biopsy specimen was obtained by video-assisted thoracoscopic surgery, which was diagnosed on pathology as a schwannoma. The hyponatremia was completely resolved after schwannoma resection and plasma ADH level decreased from 4.40 pg/mL to 0.86 pg/mL. This case highlights the importance of suspecting and identifying the underlying cause of SIADH when faced with refractory or recurrent hyponatremia, and that on possibility is mediastinal schwannoma.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


