Preserved in vitro immunoreactivity in children receiving long-term immunosuppressive therapy due to inflammatory bowel disease or autoimmune hepatitis.
{"title":"Preserved in vitro immunoreactivity in children receiving long-term immunosuppressive therapy due to inflammatory bowel disease or autoimmune hepatitis.","authors":"Teresa Schleker, Eva-Maria Jacobsen, Benjamin Mayer, Gudrun Strauss, Klaus-Michael Debatin, Carsten Posovszky","doi":"10.1186/s40348-018-0079-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Children with inflammatory bowel disease (IBD) or autoimmune hepatitis (AIH) are at risk for severe infections. This is partially a result of their chronic disease condition but, moreover, a side effect of their immunosuppressive therapy. Currently, vaccinations with live vaccines are regarded as contraindicated under immunosuppressive therapy, mainly because of concerns about side effects and a lack of data showing an adequate immune reaction. As there is no systematic study on the individual immunoreactivity under immunosuppressive therapy in this patient group, we analyzed the lymphocyte subgroups and immunoreactivity of lymphocytes in children with IBD or AIH with and without immunosuppressive therapy in vitro.</p><p><strong>Methods: </strong>We collected whole blood samples from 17 children with IBD or AIH on high-level immunosuppression (IS) (group 1) and 8 on low-level IS (group 2) in comparison with 6 patients without systemic IS (group 3). After Ficoll separation of peripheral mononuclear cells, the samples were analyzed by flow cytometry to determine the lymphocyte subgroups. Furthermore, we stimulated the isolated lymphocytes with phytohemagglutinin (PHA), tetanus antigen, and adenovirus antigen and measured their proliferation by incorporation of H<sub>3</sub>-thymidine detected in a beta counter. The statistical evaluation was performed by Kruskal-Wallis test and Mann-Whitney U test using a bilateral level of significance of α = 5%.</p><p><strong>Results: </strong>Patients with low- or high-level IS showed no significant difference in the number of lymphocytes or T cells. Interestingly, IS did not influence the lymphocyte proliferation assay significantly regarding median reaction to PHA, tetanus antigen, or adenovirus antigen between the three groups. However, comparing all immunosuppressed patients to the patients without IS, there was a significant difference towards stimulation with tetanus antigen.</p><p><strong>Conclusions: </strong>Contrary to expectations of a strong influence of IS therapy on the immunoreactivity, this study showed only minor differences between the groups with high-level, low-level, and no IS. Particularly, the in vitro reactivity to adenovirus antigen was nearly the same in all three groups. We assume that-provided a normal distribution and count of lymphocyte subgroups-patients with moderate immunosuppression might be capable of raising an effective immune response to inactivated and live vaccines.</p>","PeriodicalId":74215,"journal":{"name":"Molecular and cellular pediatrics","volume":"5 1","pages":"1"},"PeriodicalIF":2.4000,"publicationDate":"2018-01-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s40348-018-0079-0","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Molecular and cellular pediatrics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40348-018-0079-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 4
Abstract
Background: Children with inflammatory bowel disease (IBD) or autoimmune hepatitis (AIH) are at risk for severe infections. This is partially a result of their chronic disease condition but, moreover, a side effect of their immunosuppressive therapy. Currently, vaccinations with live vaccines are regarded as contraindicated under immunosuppressive therapy, mainly because of concerns about side effects and a lack of data showing an adequate immune reaction. As there is no systematic study on the individual immunoreactivity under immunosuppressive therapy in this patient group, we analyzed the lymphocyte subgroups and immunoreactivity of lymphocytes in children with IBD or AIH with and without immunosuppressive therapy in vitro.
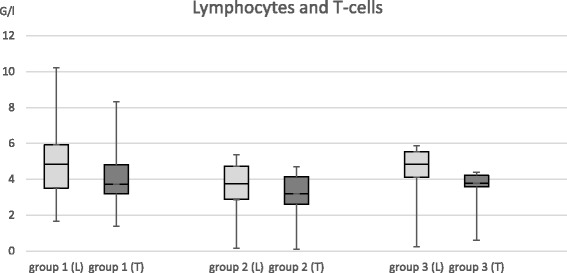
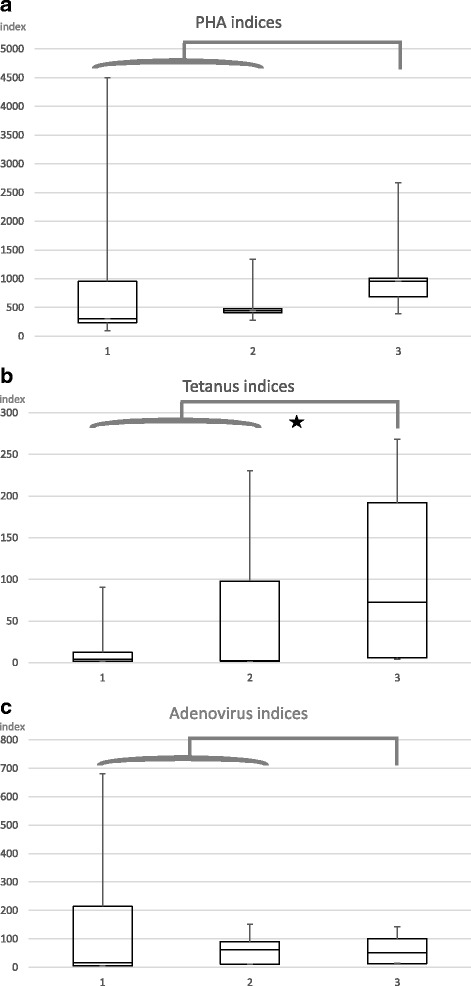
Methods: We collected whole blood samples from 17 children with IBD or AIH on high-level immunosuppression (IS) (group 1) and 8 on low-level IS (group 2) in comparison with 6 patients without systemic IS (group 3). After Ficoll separation of peripheral mononuclear cells, the samples were analyzed by flow cytometry to determine the lymphocyte subgroups. Furthermore, we stimulated the isolated lymphocytes with phytohemagglutinin (PHA), tetanus antigen, and adenovirus antigen and measured their proliferation by incorporation of H3-thymidine detected in a beta counter. The statistical evaluation was performed by Kruskal-Wallis test and Mann-Whitney U test using a bilateral level of significance of α = 5%.
Results: Patients with low- or high-level IS showed no significant difference in the number of lymphocytes or T cells. Interestingly, IS did not influence the lymphocyte proliferation assay significantly regarding median reaction to PHA, tetanus antigen, or adenovirus antigen between the three groups. However, comparing all immunosuppressed patients to the patients without IS, there was a significant difference towards stimulation with tetanus antigen.
Conclusions: Contrary to expectations of a strong influence of IS therapy on the immunoreactivity, this study showed only minor differences between the groups with high-level, low-level, and no IS. Particularly, the in vitro reactivity to adenovirus antigen was nearly the same in all three groups. We assume that-provided a normal distribution and count of lymphocyte subgroups-patients with moderate immunosuppression might be capable of raising an effective immune response to inactivated and live vaccines.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


