Ariel E Eber, Alyx Rosen, Kate E Oberlin, Alessio Giubellino, Paolo Romanelli
{"title":"Ichthyosiform Pityriasis Rubra Pilaris-Like Eruption Secondary to Ponatinib Therapy: Case Report and Literature Review.","authors":"Ariel E Eber, Alyx Rosen, Kate E Oberlin, Alessio Giubellino, Paolo Romanelli","doi":"10.1007/s40800-017-0055-y","DOIUrl":null,"url":null,"abstract":"<p><p>Tyrosine kinase inhibitors have revolutionized the chemotherapy arena as targeted therapies for a multitude of malignancies. They are more selective than conventional chemotherapy, and often elicit fewer systemic adverse events, however toxicities still exist. Cutaneous toxicities are common and their management presents a novel challenge to physicians and patients. Ponatinib is a third-generation tyrosine kinase inhibitor increasingly reported to cause cutaneous eruption. A 50-year-old woman with a history of chronic myelogenous leukemia presented with a 4-month history of worsening atrophic and ichthyosiform pink plaques involving the axillae, thighs and abdomen; red patches were also observed on the cheeks and forehead. She was started on the third-generation, ponatinib, 5 months earlier because of disease refractory to previous therapies including interferon, imatinib, dasatinib and bosutinib. A skin biopsy revealed perifollicular fibrosis, alternating orthokeratosis and parakeratosis, and a sparse perivascular lymphocytic infiltrate consistent with a pityriasis rubra pilaris-like reaction. Topical tretinoin 0.025% cream was initiated, resulting in resolution within 3 weeks without discontinuation of ponatinib. A review of previous reports identified significant similarities among the ponatinib-induced drug reactions. Here, we highlight not only that cutaneous eruptions occur on ponatinib therapy, but that the dermatologic manifestations are characteristic and unique, and benefit from retinoid therapy, without requiring interruption of vital chemotherapy.</p>","PeriodicalId":11364,"journal":{"name":"Drug Safety - Case Reports","volume":"4 1","pages":"19"},"PeriodicalIF":0.0000,"publicationDate":"2017-11-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1007/s40800-017-0055-y","citationCount":"17","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drug Safety - Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s40800-017-0055-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 17
Abstract
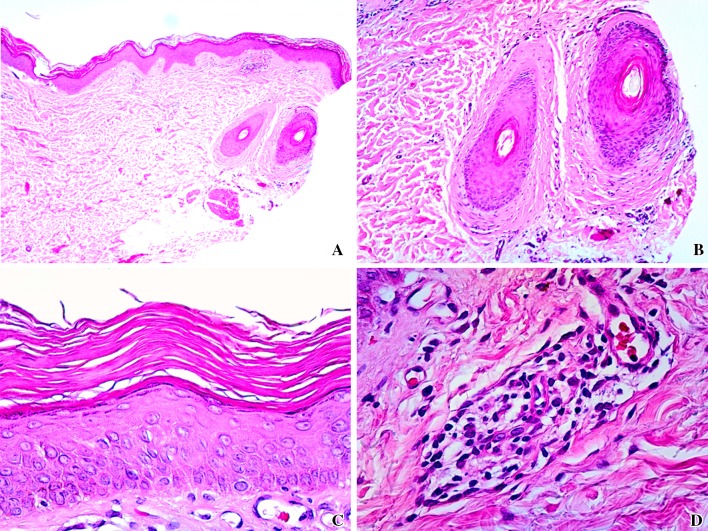
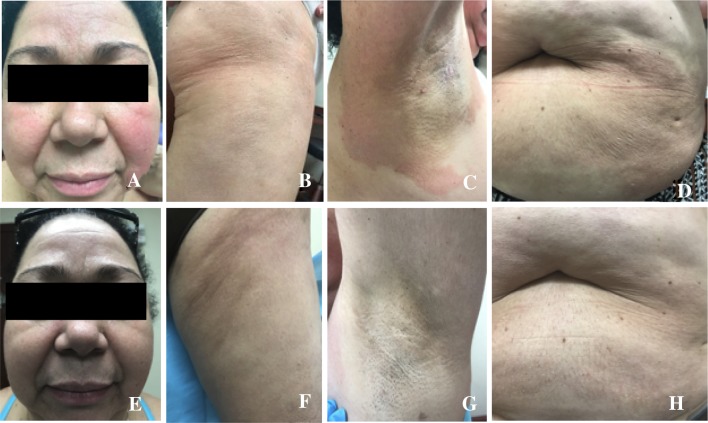
Tyrosine kinase inhibitors have revolutionized the chemotherapy arena as targeted therapies for a multitude of malignancies. They are more selective than conventional chemotherapy, and often elicit fewer systemic adverse events, however toxicities still exist. Cutaneous toxicities are common and their management presents a novel challenge to physicians and patients. Ponatinib is a third-generation tyrosine kinase inhibitor increasingly reported to cause cutaneous eruption. A 50-year-old woman with a history of chronic myelogenous leukemia presented with a 4-month history of worsening atrophic and ichthyosiform pink plaques involving the axillae, thighs and abdomen; red patches were also observed on the cheeks and forehead. She was started on the third-generation, ponatinib, 5 months earlier because of disease refractory to previous therapies including interferon, imatinib, dasatinib and bosutinib. A skin biopsy revealed perifollicular fibrosis, alternating orthokeratosis and parakeratosis, and a sparse perivascular lymphocytic infiltrate consistent with a pityriasis rubra pilaris-like reaction. Topical tretinoin 0.025% cream was initiated, resulting in resolution within 3 weeks without discontinuation of ponatinib. A review of previous reports identified significant similarities among the ponatinib-induced drug reactions. Here, we highlight not only that cutaneous eruptions occur on ponatinib therapy, but that the dermatologic manifestations are characteristic and unique, and benefit from retinoid therapy, without requiring interruption of vital chemotherapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


