Su Woong Jung, Eun Ji Park, Jin Sug Kim, Tae Won Lee, Chun Gyoo Ihm, Sang Ho Lee, Ju-Young Moon, Yang Gyun Kim, Kyung Hwan Jeong
{"title":"Renal Tubular Acidosis in Patients with Primary Sjögren's Syndrome.","authors":"Su Woong Jung, Eun Ji Park, Jin Sug Kim, Tae Won Lee, Chun Gyoo Ihm, Sang Ho Lee, Ju-Young Moon, Yang Gyun Kim, Kyung Hwan Jeong","doi":"10.5049/EBP.2017.15.1.17","DOIUrl":null,"url":null,"abstract":"<p><p>Primary Sjögren's syndrome (pSS) is characterized by lymphocytic infiltration of the exocrine glands resulting in decreased saliva and tear production. It uncommonly involves the kidneys in various forms, including tubulointerstitial nephritis, renal tubular acidosis, Fanconi syndrome, and rarely glomerulonephritis. Its clinical symptoms include muscle weakness, periodic paralysis, and bone pain due to metabolic acidosis and electrolyte imbalance. Herein, we describe the cases of two women with pSS whose presenting symptoms involve the kidneys. They had hypokalemia and normal anion gap metabolic acidosis due to distal renal tubular acidosis and positive anti-SS-A and anti-SS-B autoantibodies. Since one of them experienced femoral fracture due to osteomalacia secondary to renal tubular acidosis, an earlier diagnosis of pSS is important in preventing serious complications.</p>","PeriodicalId":35352,"journal":{"name":"Electrolyte and Blood Pressure","volume":"15 1","pages":"17-22"},"PeriodicalIF":0.0000,"publicationDate":"2017-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.5049/EBP.2017.15.1.17","citationCount":"19","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Electrolyte and Blood Pressure","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5049/EBP.2017.15.1.17","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/9/30 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 19
Abstract
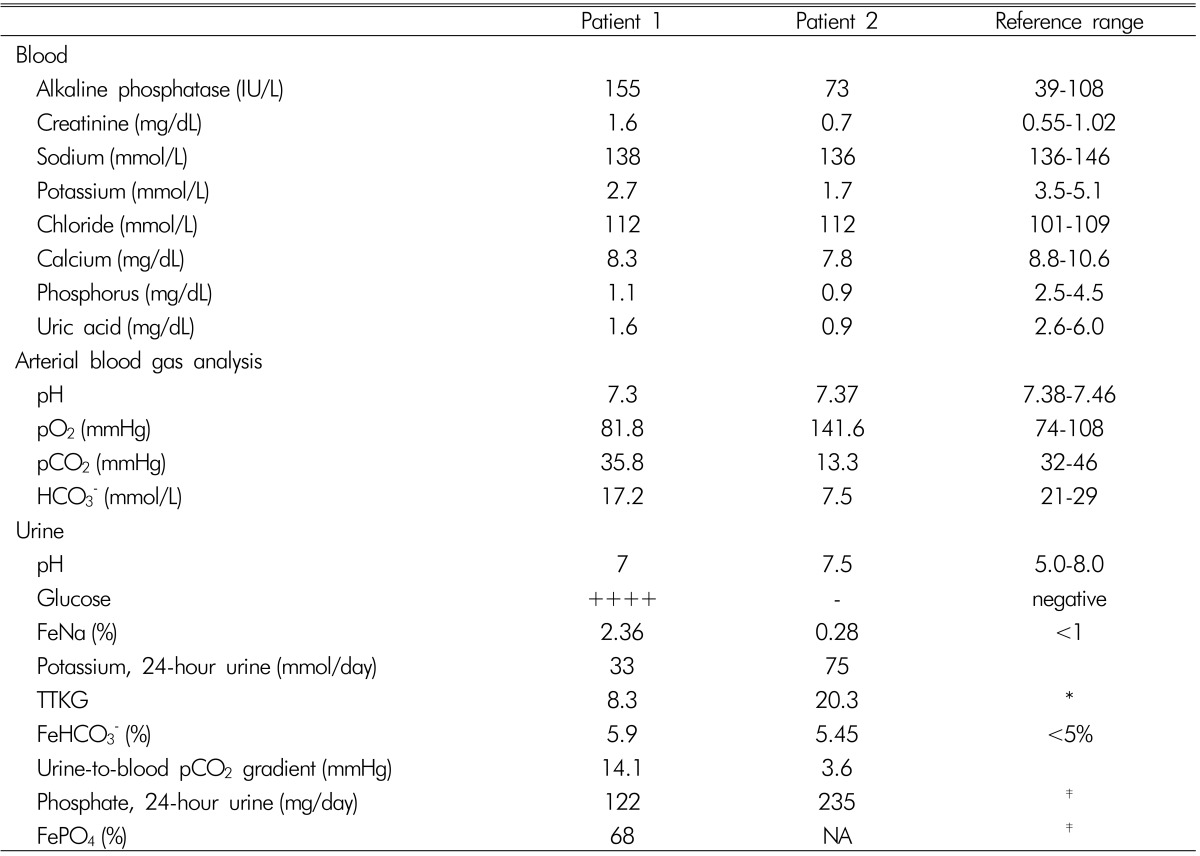
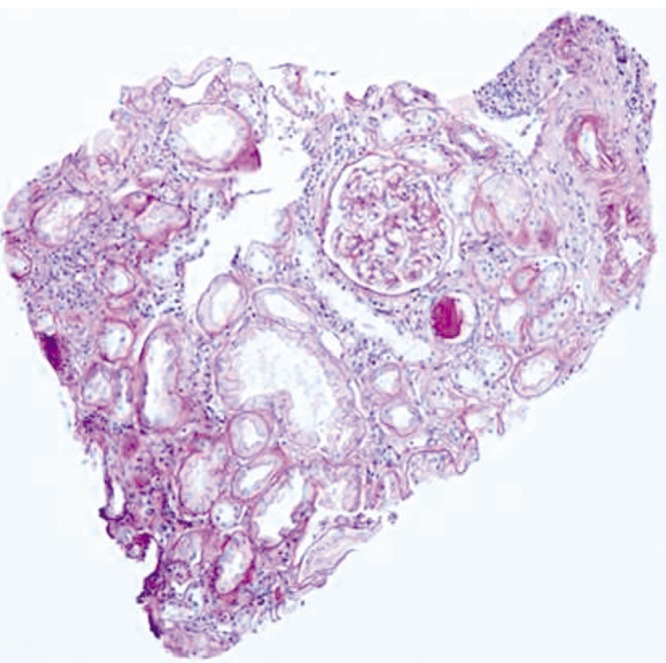
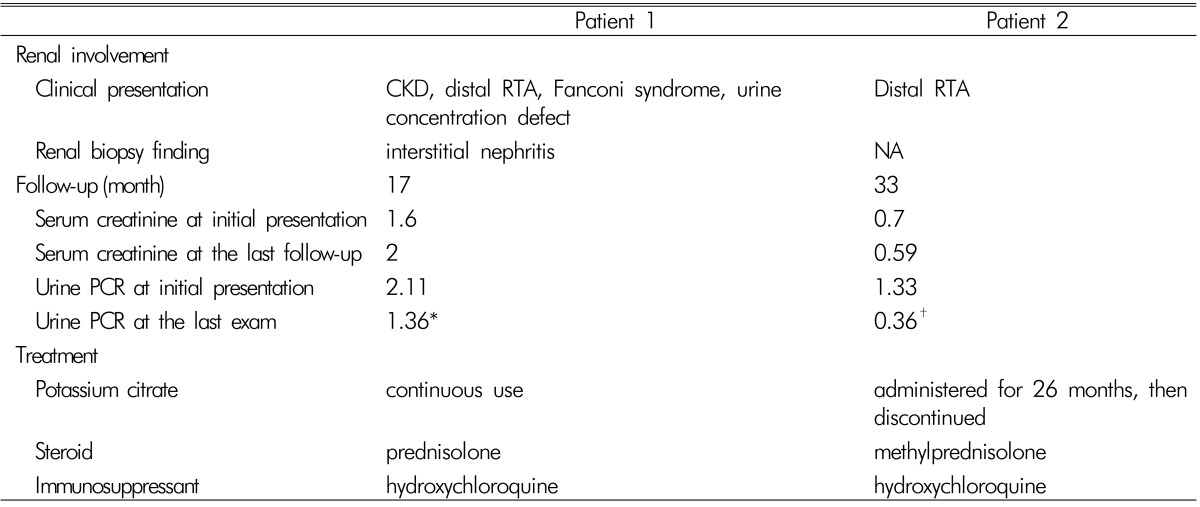
Primary Sjögren's syndrome (pSS) is characterized by lymphocytic infiltration of the exocrine glands resulting in decreased saliva and tear production. It uncommonly involves the kidneys in various forms, including tubulointerstitial nephritis, renal tubular acidosis, Fanconi syndrome, and rarely glomerulonephritis. Its clinical symptoms include muscle weakness, periodic paralysis, and bone pain due to metabolic acidosis and electrolyte imbalance. Herein, we describe the cases of two women with pSS whose presenting symptoms involve the kidneys. They had hypokalemia and normal anion gap metabolic acidosis due to distal renal tubular acidosis and positive anti-SS-A and anti-SS-B autoantibodies. Since one of them experienced femoral fracture due to osteomalacia secondary to renal tubular acidosis, an earlier diagnosis of pSS is important in preventing serious complications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


