E Panther, B Lucke-Wold, D Laurent, C Osorno-Cruz, Y Mehkri, R Turner, A Polifka, M Koch, B Hoh, N Chalouhi
{"title":"Treatment of Dissecting Vertebral Pseudoaneurysms: A Single-Center Experience.","authors":"E Panther, B Lucke-Wold, D Laurent, C Osorno-Cruz, Y Mehkri, R Turner, A Polifka, M Koch, B Hoh, N Chalouhi","doi":"","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Dissecting vertebral artery pseudoaneurysms represent a unique clinical challenge with careful appreciation for location of the posterior inferior cerebellar artery. Limited data is available in terms of outcomes regarding the various treatment modalities.</p><p><strong>Methods: </strong>11 patients with dissecting pseudoaneurysms were identified from 2013-2021. Pseudoaneurysm size and morphology, clinical presentation, and treatment approach was collected. Success of treatment was recorded based on post-operative imaging as well as documented overall patient outcomes. Three primary treatment modalities emerged: coil embolization, stent assisted coiling, and flow diversion.</p><p><strong>Results: </strong>Of the 11 patients, 5 were female and 6 were male with an age from 36 to 69.7. 7 had ruptured pseudoaneurysms at time of treatment. Size of pseudoaneurysm ranged from 3 to 6 mm. 8 were on the right and 3 were on the left vertebral artery. 8 were proximal to PICA and 3 were distal. Co-dominance of vertebral filling was seen in 5 patients, 5 with dominance through right vertebral artery, and 1 with dominance through left vertebral artery. Variability existed in treatment approaches with 4 patients undergoing coil occlusion, 5 patients undergoing flow diversion stenting, and 2 patients undergoing flow diversion stenting with jailed coiling. 1 patient had enlargement of pseudoaneurysm while inpatient and required a second flow diversion device. 1 patient had two flow diversion devices placed initially at time of treatment due to morphology of PA. 6 patients had repeat angiograms between 6 to 9 months with complete occlusion. 3 had CTA or MRA with complete occlusion for those that had flow diversion, they were transitioned from aspirin and clopidogrel to aspirin monotherapy after first repeat angiogram. 6 patients required shunt placement for hydrocephalus. 1 patient died prior to discharge due to sepsis. 2 patients died post discharge: 1 with myocardial infarction and the 2nd due to urosepsis.Dissecting vertebral pseudoaneurysm has high morbidity and mortality if rupture occurs. Location of PICA origin influences treatment approach. Patients with poor Hunt/Hess scores upon arrival had increased risk for systemic infection and mortality.</p>","PeriodicalId":92000,"journal":{"name":"Annals of neurology and neuroscience","volume":"1 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of neurology and neuroscience","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/9/12 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Dissecting vertebral artery pseudoaneurysms represent a unique clinical challenge with careful appreciation for location of the posterior inferior cerebellar artery. Limited data is available in terms of outcomes regarding the various treatment modalities.
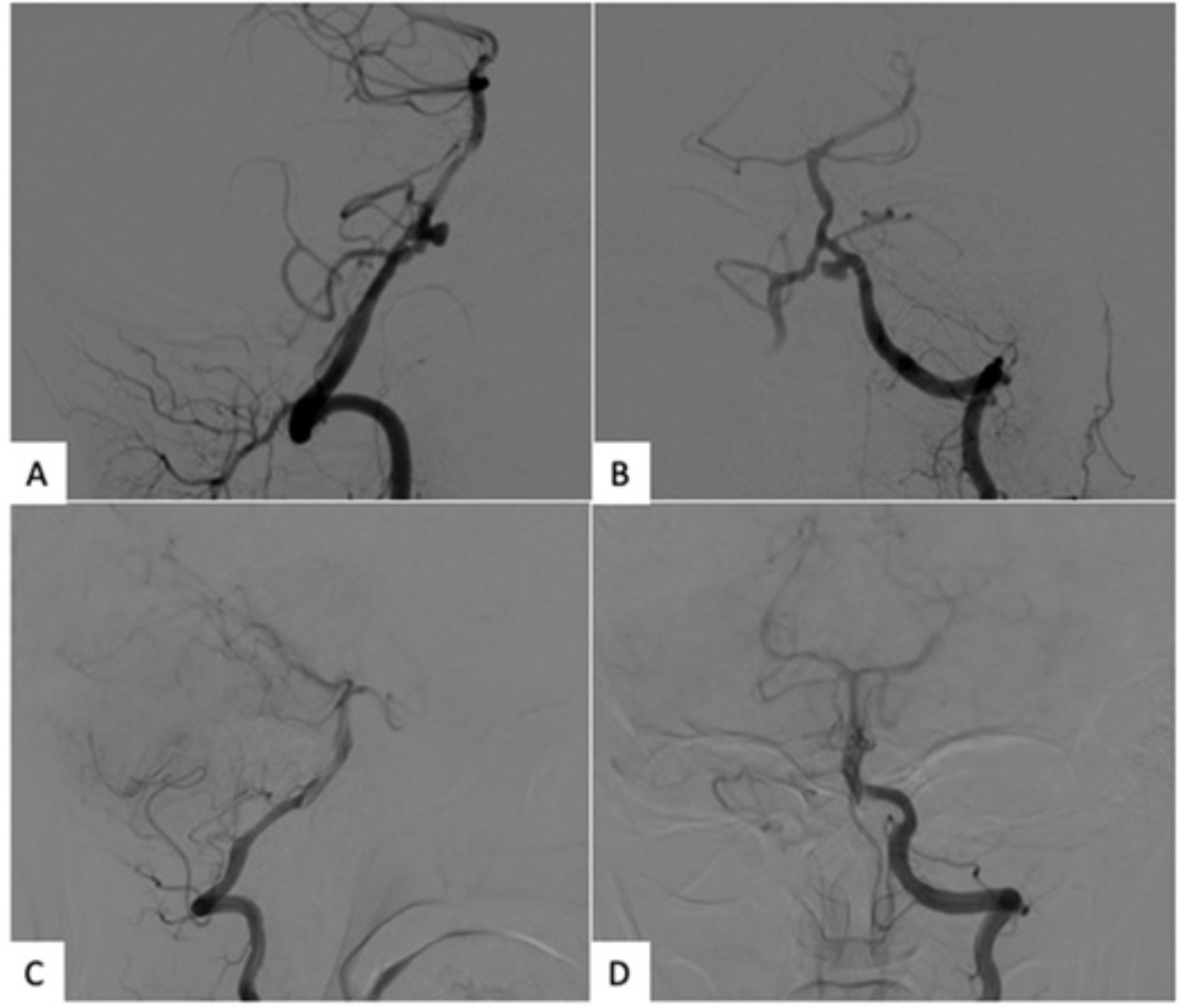
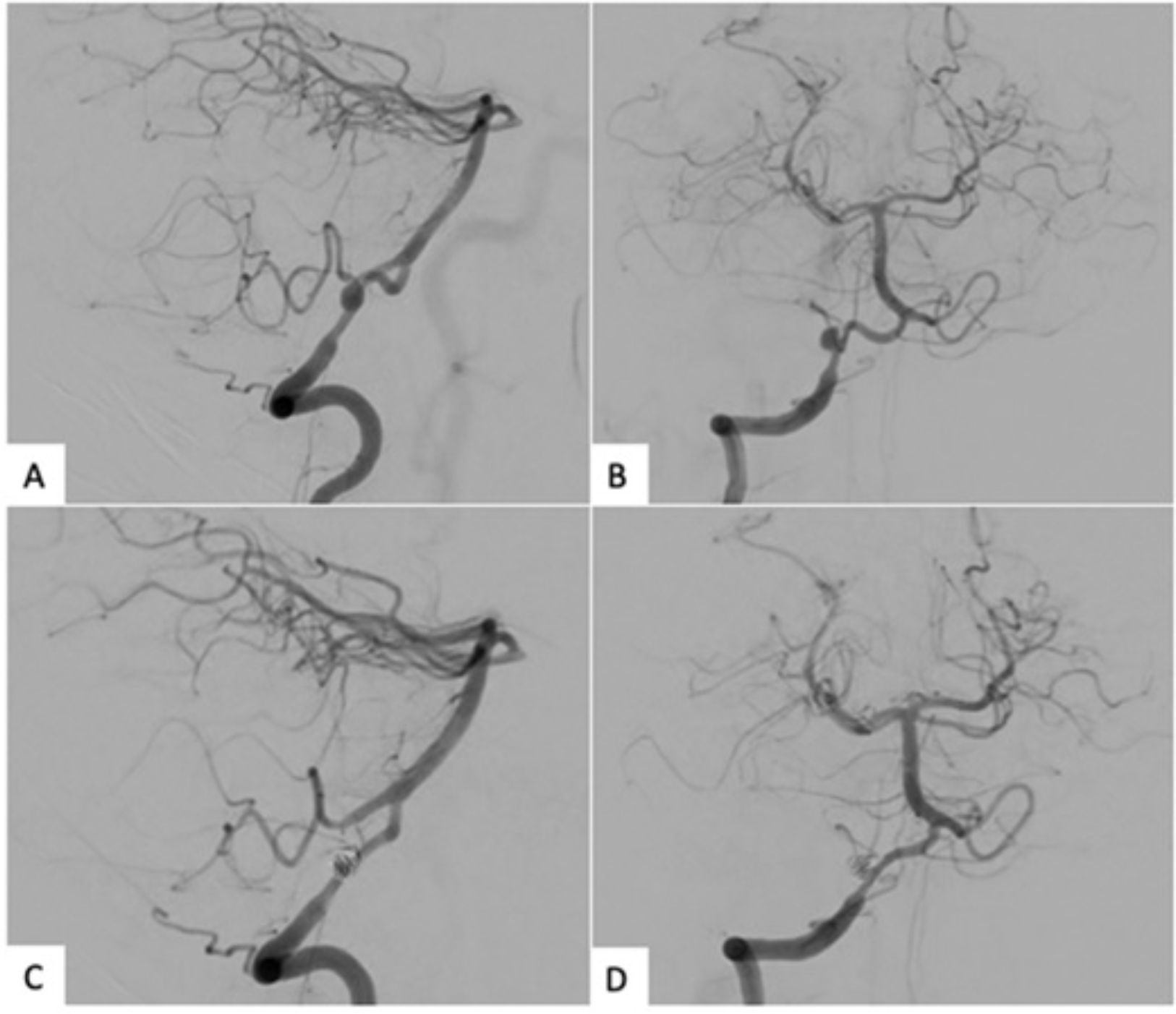
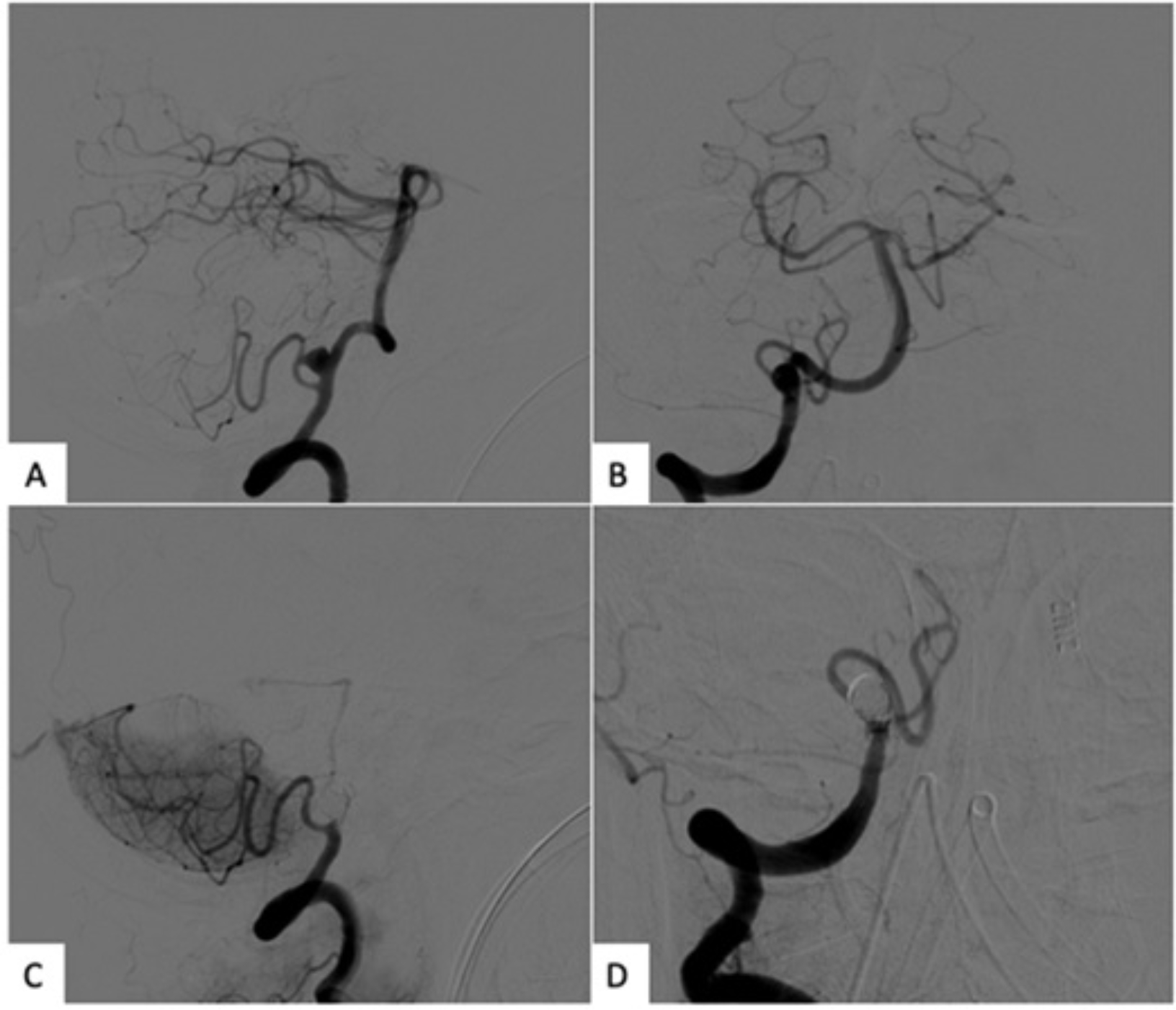
Methods: 11 patients with dissecting pseudoaneurysms were identified from 2013-2021. Pseudoaneurysm size and morphology, clinical presentation, and treatment approach was collected. Success of treatment was recorded based on post-operative imaging as well as documented overall patient outcomes. Three primary treatment modalities emerged: coil embolization, stent assisted coiling, and flow diversion.
Results: Of the 11 patients, 5 were female and 6 were male with an age from 36 to 69.7. 7 had ruptured pseudoaneurysms at time of treatment. Size of pseudoaneurysm ranged from 3 to 6 mm. 8 were on the right and 3 were on the left vertebral artery. 8 were proximal to PICA and 3 were distal. Co-dominance of vertebral filling was seen in 5 patients, 5 with dominance through right vertebral artery, and 1 with dominance through left vertebral artery. Variability existed in treatment approaches with 4 patients undergoing coil occlusion, 5 patients undergoing flow diversion stenting, and 2 patients undergoing flow diversion stenting with jailed coiling. 1 patient had enlargement of pseudoaneurysm while inpatient and required a second flow diversion device. 1 patient had two flow diversion devices placed initially at time of treatment due to morphology of PA. 6 patients had repeat angiograms between 6 to 9 months with complete occlusion. 3 had CTA or MRA with complete occlusion for those that had flow diversion, they were transitioned from aspirin and clopidogrel to aspirin monotherapy after first repeat angiogram. 6 patients required shunt placement for hydrocephalus. 1 patient died prior to discharge due to sepsis. 2 patients died post discharge: 1 with myocardial infarction and the 2nd due to urosepsis.Dissecting vertebral pseudoaneurysm has high morbidity and mortality if rupture occurs. Location of PICA origin influences treatment approach. Patients with poor Hunt/Hess scores upon arrival had increased risk for systemic infection and mortality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


