Effects of Strong CYP3A Inhibition and Induction on the Pharmacokinetics of Ixazomib, an Oral Proteasome Inhibitor: Results of Drug-Drug Interaction Studies in Patients With Advanced Solid Tumors or Lymphoma and a Physiologically Based Pharmacokinetic Analysis.
Neeraj Gupta, Michael J Hanley, Karthik Venkatakrishnan, Alberto Bessudo, Drew W Rasco, Sunil Sharma, Bert H O'Neil, Bingxia Wang, Guohui Liu, Alice Ke, Chirag Patel, Karen Rowland Yeo, Cindy Xia, Xiaoquan Zhang, Dixie-Lee Esseltine, John Nemunaitis
{"title":"Effects of Strong CYP3A Inhibition and Induction on the Pharmacokinetics of Ixazomib, an Oral Proteasome Inhibitor: Results of Drug-Drug Interaction Studies in Patients With Advanced Solid Tumors or Lymphoma and a Physiologically Based Pharmacokinetic Analysis.","authors":"Neeraj Gupta, Michael J Hanley, Karthik Venkatakrishnan, Alberto Bessudo, Drew W Rasco, Sunil Sharma, Bert H O'Neil, Bingxia Wang, Guohui Liu, Alice Ke, Chirag Patel, Karen Rowland Yeo, Cindy Xia, Xiaoquan Zhang, Dixie-Lee Esseltine, John Nemunaitis","doi":"10.1002/jcph.988","DOIUrl":null,"url":null,"abstract":"<p><p>At clinically relevant ixazomib concentrations, in vitro studies demonstrated that no specific cytochrome P450 (CYP) enzyme predominantly contributes to ixazomib metabolism. However, at higher than clinical concentrations, ixazomib was metabolized by multiple CYP isoforms, with the estimated relative contribution being highest for CYP3A at 42%. This multiarm phase 1 study (Clinicaltrials.gov identifier: NCT01454076) investigated the effect of the strong CYP3A inhibitors ketoconazole and clarithromycin and the strong CYP3A inducer rifampin on the pharmacokinetics of ixazomib. Eighty-eight patients were enrolled across the 3 drug-drug interaction studies; the ixazomib toxicity profile was consistent with previous studies. Ketoconazole and clarithromycin had no clinically meaningful effects on the pharmacokinetics of ixazomib. The geometric least-squares mean area under the plasma concentration-time curve from 0 to 264 hours postdose ratio (90%CI) with vs without ketoconazole coadministration was 1.09 (0.91-1.31) and was 1.11 (0.86-1.43) with vs without clarithromycin coadministration. Reduced plasma exposures of ixazomib were observed following coadministration with rifampin. Ixazomib area under the plasma concentration-time curve from time 0 to the time of the last quantifiable concentration was reduced by 74% (geometric least-squares mean ratio of 0.26 [90%CI 0.18-0.37]), and maximum observed plasma concentration was reduced by 54% (geometric least-squares mean ratio of 0.46 [90%CI 0.29-0.73]) in the presence of rifampin. The clinical drug-drug interaction study results were reconciled well by a physiologically based pharmacokinetic model that incorporated a minor contribution of CYP3A to overall ixazomib clearance and quantitatively considered the strength of induction of CYP3A and intestinal P-glycoprotein by rifampin. On the basis of these study results, the ixazomib prescribing information recommends that patients should avoid concomitant administration of strong CYP3A inducers with ixazomib.</p>","PeriodicalId":15536,"journal":{"name":"Journal of clinical pharmacology","volume":"58 2","pages":"180-192"},"PeriodicalIF":2.3000,"publicationDate":"2018-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1002/jcph.988","citationCount":"34","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of clinical pharmacology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/jcph.988","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/8/11 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 34
Abstract
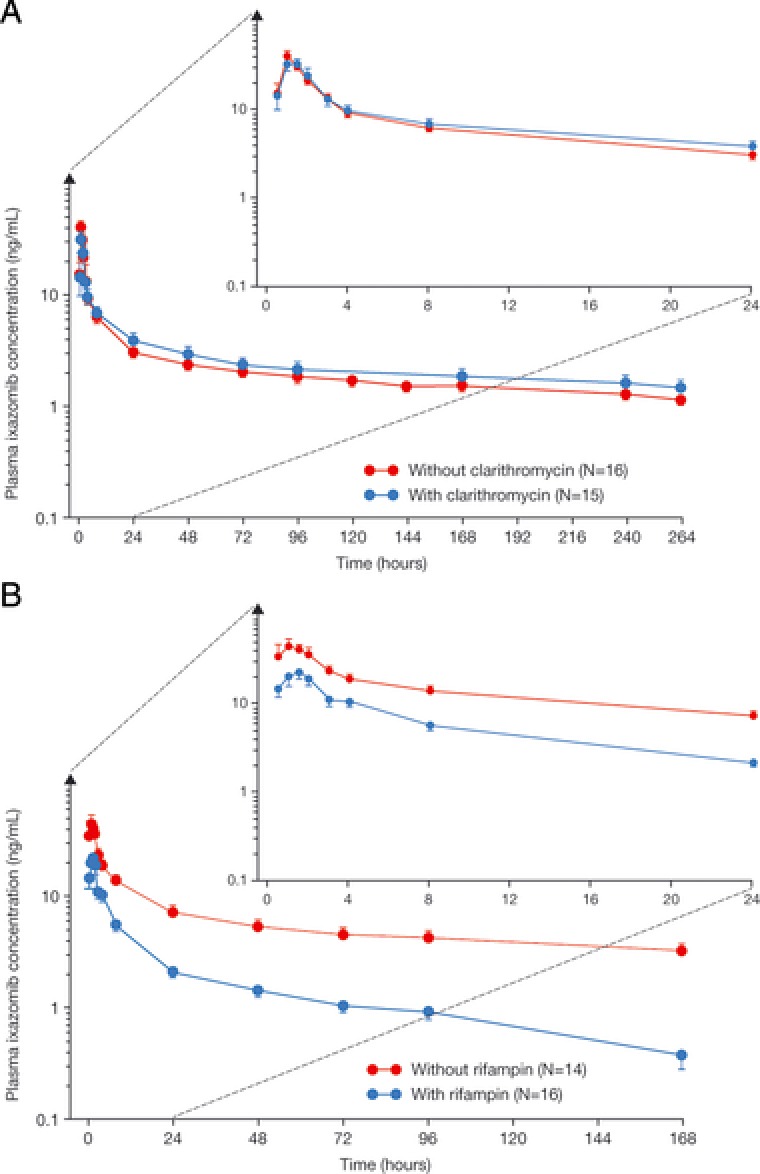
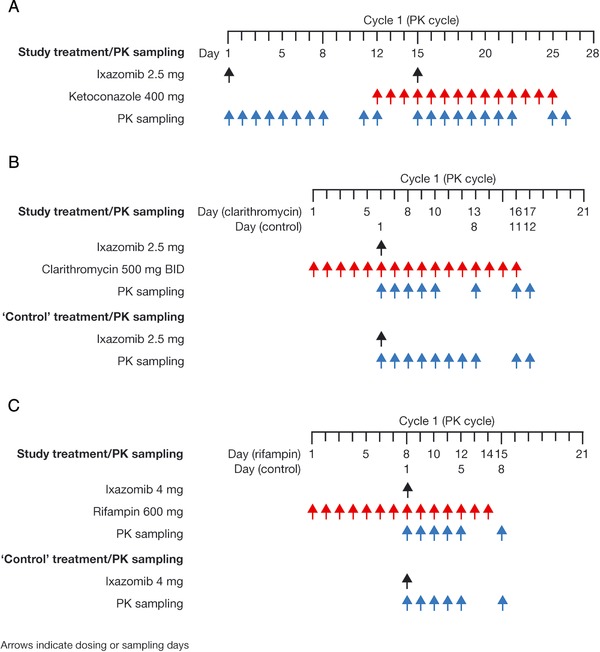
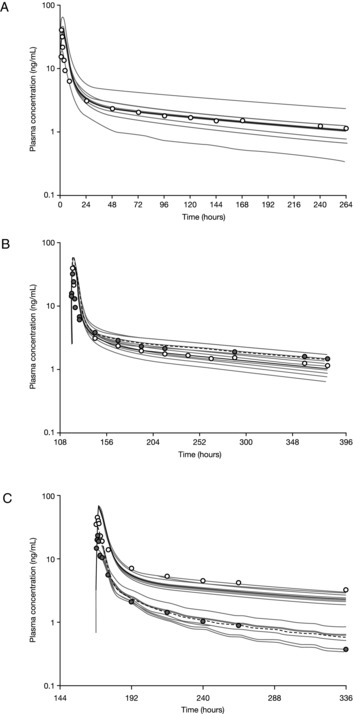
At clinically relevant ixazomib concentrations, in vitro studies demonstrated that no specific cytochrome P450 (CYP) enzyme predominantly contributes to ixazomib metabolism. However, at higher than clinical concentrations, ixazomib was metabolized by multiple CYP isoforms, with the estimated relative contribution being highest for CYP3A at 42%. This multiarm phase 1 study (Clinicaltrials.gov identifier: NCT01454076) investigated the effect of the strong CYP3A inhibitors ketoconazole and clarithromycin and the strong CYP3A inducer rifampin on the pharmacokinetics of ixazomib. Eighty-eight patients were enrolled across the 3 drug-drug interaction studies; the ixazomib toxicity profile was consistent with previous studies. Ketoconazole and clarithromycin had no clinically meaningful effects on the pharmacokinetics of ixazomib. The geometric least-squares mean area under the plasma concentration-time curve from 0 to 264 hours postdose ratio (90%CI) with vs without ketoconazole coadministration was 1.09 (0.91-1.31) and was 1.11 (0.86-1.43) with vs without clarithromycin coadministration. Reduced plasma exposures of ixazomib were observed following coadministration with rifampin. Ixazomib area under the plasma concentration-time curve from time 0 to the time of the last quantifiable concentration was reduced by 74% (geometric least-squares mean ratio of 0.26 [90%CI 0.18-0.37]), and maximum observed plasma concentration was reduced by 54% (geometric least-squares mean ratio of 0.46 [90%CI 0.29-0.73]) in the presence of rifampin. The clinical drug-drug interaction study results were reconciled well by a physiologically based pharmacokinetic model that incorporated a minor contribution of CYP3A to overall ixazomib clearance and quantitatively considered the strength of induction of CYP3A and intestinal P-glycoprotein by rifampin. On the basis of these study results, the ixazomib prescribing information recommends that patients should avoid concomitant administration of strong CYP3A inducers with ixazomib.
期刊介绍:
The Journal of Clinical Pharmacology (JCP) is a Human Pharmacology journal designed to provide physicians, pharmacists, research scientists, regulatory scientists, drug developers and academic colleagues a forum to present research in all aspects of Clinical Pharmacology. This includes original research in pharmacokinetics, pharmacogenetics/pharmacogenomics, pharmacometrics, physiologic based pharmacokinetic modeling, drug interactions, therapeutic drug monitoring, regulatory sciences (including unique methods of data analysis), special population studies, drug development, pharmacovigilance, womens’ health, pediatric pharmacology, and pharmacodynamics. Additionally, JCP publishes review articles, commentaries and educational manuscripts. The Journal also serves as an instrument to disseminate Public Policy statements from the American College of Clinical Pharmacology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


