Ovidiu Vasile Bochis, Zsolt Fekete, Catalin Vlad, Bogdan Fetica, Daniel Corneliu Leucuta, Constantin Ioan Busuioc, Alexandru Irimie
{"title":"The importance of a multidisciplinary team in rectal cancer management.","authors":"Ovidiu Vasile Bochis, Zsolt Fekete, Catalin Vlad, Bogdan Fetica, Daniel Corneliu Leucuta, Constantin Ioan Busuioc, Alexandru Irimie","doi":"10.15386/cjmed-689","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The aim of this study was to evaluate the impact of the interval between surgery and adjuvant treatments regarding the overall survival and recurrence-free survival in patients from a developing country. For stages II and III rectal cancer, international guidelines recommend neoadjuvant chemoradiotherapy (CRT) regardless of the tumor location. In the developing countries there is a shortage of radiotherapy centers, specialists, which lead to long waiting lists for radiotherapy. These problems might lead to protocol deviations.</p><p><strong>Methods: </strong>We conducted a retrospective study on 161 patients with rectal cancer treated with surgery, postoperative CRT and with or without chemotherapy for a total of 6 months, at The Oncology Institute Cluj-Napoca between 2006-2010. All patients had 5 years of follow-up.</p><p><strong>Results: </strong>A total of 161 patients were enrolled in this study. The majority of patients were locally advanced stages (89.44%). The well known prognostic factors, such as TNM stage, performance status, CEA serum level, perineural, vascular and lymphatic invasion, and node capsular effraction had a statistically significant influence on overall survival. In 21.12% of patients the first adjuvant treatment was started in the first 4 weeks after surgery. Only 13.04% of patients started the concomitant CRT within the limit of 6 weeks after surgery. Concerning the time between surgery and CRT, we did not observe a statistically significantly difference in OS if the radiotherapy started after the first 6 weeks (p=0.701). The OS rate for locally advanced rectal cancer patients was 69.44%.</p><p><strong>Conclusions: </strong>In rectal cancer, the importance of the first therapeutic act is crucial. Following international guidelines provides a survival advantage and a better quality of life. In case of adjuvant treatment, it is recommended to start this treatment as soon as the local infrastructure allows it.</p>","PeriodicalId":91233,"journal":{"name":"Clujul medical (1957)","volume":"90 3","pages":"279-285"},"PeriodicalIF":0.0000,"publicationDate":"2017-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/39/47/cm-90-279.PMC5536207.pdf","citationCount":"5","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clujul medical (1957)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15386/cjmed-689","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/7/15 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 5
Abstract
Introduction: The aim of this study was to evaluate the impact of the interval between surgery and adjuvant treatments regarding the overall survival and recurrence-free survival in patients from a developing country. For stages II and III rectal cancer, international guidelines recommend neoadjuvant chemoradiotherapy (CRT) regardless of the tumor location. In the developing countries there is a shortage of radiotherapy centers, specialists, which lead to long waiting lists for radiotherapy. These problems might lead to protocol deviations.
Methods: We conducted a retrospective study on 161 patients with rectal cancer treated with surgery, postoperative CRT and with or without chemotherapy for a total of 6 months, at The Oncology Institute Cluj-Napoca between 2006-2010. All patients had 5 years of follow-up.
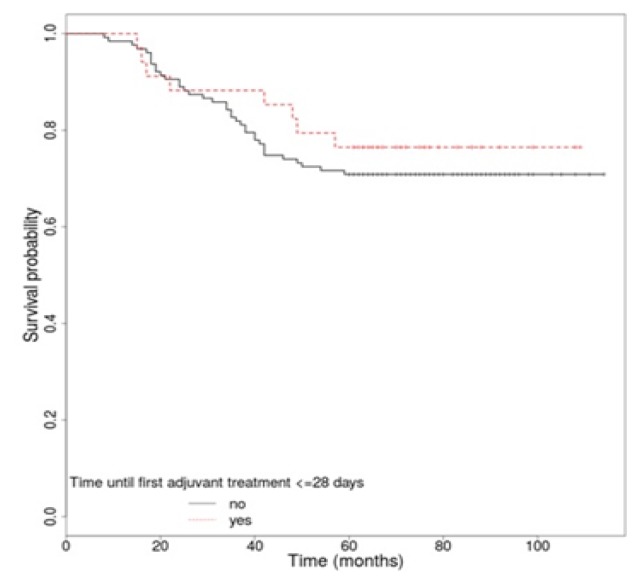
Results: A total of 161 patients were enrolled in this study. The majority of patients were locally advanced stages (89.44%). The well known prognostic factors, such as TNM stage, performance status, CEA serum level, perineural, vascular and lymphatic invasion, and node capsular effraction had a statistically significant influence on overall survival. In 21.12% of patients the first adjuvant treatment was started in the first 4 weeks after surgery. Only 13.04% of patients started the concomitant CRT within the limit of 6 weeks after surgery. Concerning the time between surgery and CRT, we did not observe a statistically significantly difference in OS if the radiotherapy started after the first 6 weeks (p=0.701). The OS rate for locally advanced rectal cancer patients was 69.44%.
Conclusions: In rectal cancer, the importance of the first therapeutic act is crucial. Following international guidelines provides a survival advantage and a better quality of life. In case of adjuvant treatment, it is recommended to start this treatment as soon as the local infrastructure allows it.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


