Nikolas Rae, Aran Singanayagam, Stuart Schembri, James D Chalmers
{"title":"Oral versus intravenous clarithromycin in moderate to severe community-acquired pneumonia: an observational study.","authors":"Nikolas Rae, Aran Singanayagam, Stuart Schembri, James D Chalmers","doi":"10.1186/s41479-017-0025-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>British Thoracic Society guidelines recommend clarithromycin in addition to beta-lactam antibiotics for patients with community-acquired pneumonia and CURB-65 score 2-5. Intravenous therapy is commonly used but there are few data on whether oral therapy is equally effective.</p><p><strong>Methods: </strong>This observational study used propensity matching to compare two groups of patients with moderate to severe community-acquired pneumonia (CURB-65 score 2-5) treated with oral (<i>n</i> = 226) or intravenous (<i>n</i> = 226) clarithromycin on admission. Outcomes were 30-day mortality, intensive care unit admission, time to clinical stability, and length of hospital stay.</p><p><strong>Results: </strong>There was no significant difference in 30-day mortality (16.8% for intravenous [IV] group vs. 14.6% for oral group, hazard ratio for IV group 1.11 95% CI 0.70-1.78), ICU admission (10.6% in both groups) or complications (10.6% for IV group and 9.3% for oral group) between the groups. The time to clinical stability in both cohorts was a median of 5 days (interquartile range 3-7 days, <i>p</i> = 0.3). The median length of hospital stay was 8 days in the IV group (interquartile range 4-14 days) and 7 days in the oral group (interquartile range 4-13 days), <i>p</i> = 0.5. No other differences were observed between oral and IV groups.</p><p><strong>Conclusion: </strong>Where the oral route is not compromised, oral macrolides appear to be equivalent to IV in treating moderate to severe CAP.</p>","PeriodicalId":45120,"journal":{"name":"Pneumonia","volume":"9 ","pages":"2"},"PeriodicalIF":8.5000,"publicationDate":"2017-02-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s41479-017-0025-2","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pneumonia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41479-017-0025-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 3
Abstract
Objectives: British Thoracic Society guidelines recommend clarithromycin in addition to beta-lactam antibiotics for patients with community-acquired pneumonia and CURB-65 score 2-5. Intravenous therapy is commonly used but there are few data on whether oral therapy is equally effective.
Methods: This observational study used propensity matching to compare two groups of patients with moderate to severe community-acquired pneumonia (CURB-65 score 2-5) treated with oral (n = 226) or intravenous (n = 226) clarithromycin on admission. Outcomes were 30-day mortality, intensive care unit admission, time to clinical stability, and length of hospital stay.
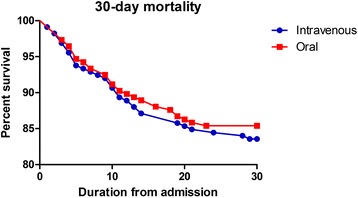
Results: There was no significant difference in 30-day mortality (16.8% for intravenous [IV] group vs. 14.6% for oral group, hazard ratio for IV group 1.11 95% CI 0.70-1.78), ICU admission (10.6% in both groups) or complications (10.6% for IV group and 9.3% for oral group) between the groups. The time to clinical stability in both cohorts was a median of 5 days (interquartile range 3-7 days, p = 0.3). The median length of hospital stay was 8 days in the IV group (interquartile range 4-14 days) and 7 days in the oral group (interquartile range 4-13 days), p = 0.5. No other differences were observed between oral and IV groups.
Conclusion: Where the oral route is not compromised, oral macrolides appear to be equivalent to IV in treating moderate to severe CAP.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


