Kathryn B Holroyd, Elias S Sotirchos, Scott R DeBoer, Kelly A Mills, Scott D Newsome
{"title":"JC virus granule cell neuronopathy onset two months after chemotherapy for low-grade lymphoma.","authors":"Kathryn B Holroyd, Elias S Sotirchos, Scott R DeBoer, Kelly A Mills, Scott D Newsome","doi":"10.1186/s40673-017-0066-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Granule cell neuronopathy (GCN) is a rare disease caused by the JC virus, leading to degeneration of cerebellar granule cell neurons. Primarily described in patients with AIDS, it has also been diagnosed in patients with lymphoproliferative diseases and after long-term treatment with immune-suppressing medications such as natalizumab.</p><p><strong>Case presentation: </strong>A 69 year old woman presented with progressive ataxia which began 2 months after initiation of treatment for follicular low-grade B cell lymphoma with rituximab/bendamustine, and progressed for 2 years prior to admission. Extensive prior evaluation included MRI that showed atrophy of the cerebellum but normal CSF analysis and serum studies. Neurologic exam on admission was notable for severe appendicular ataxia and fatigable end-gaze direction-changing horizontal nystagmus. FDG-PET/CT scan was unremarkable and repeat lumbar puncture revealed 2 WBCs/mm<sup>3</sup>, 148 RBCs/mm<sup>3</sup>, glucose 70 mg/dL, protein 37.7 mg/dL and negative flow cytometry/cytopathology. Standard CSF JC virus PCR testing was negative, but ultrasensitive TaqMan real-time JC virus PCR testing was positive, consistent with JC virus-related GCN.</p><p><strong>Conclusions: </strong>Because of the diagnostic challenges in identifying GCN, a high threshold of suspicion should be maintained in patients with an immune-suppressing condition such as lymphoma or on immune-suppressing agents such as rituximab, even shortly after initiation of therapy.</p>","PeriodicalId":36752,"journal":{"name":"Cerebellum and Ataxias","volume":"4 ","pages":"8"},"PeriodicalIF":0.0000,"publicationDate":"2017-06-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s40673-017-0066-6","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cerebellum and Ataxias","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40673-017-0066-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Granule cell neuronopathy (GCN) is a rare disease caused by the JC virus, leading to degeneration of cerebellar granule cell neurons. Primarily described in patients with AIDS, it has also been diagnosed in patients with lymphoproliferative diseases and after long-term treatment with immune-suppressing medications such as natalizumab.
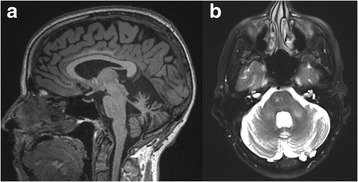
Case presentation: A 69 year old woman presented with progressive ataxia which began 2 months after initiation of treatment for follicular low-grade B cell lymphoma with rituximab/bendamustine, and progressed for 2 years prior to admission. Extensive prior evaluation included MRI that showed atrophy of the cerebellum but normal CSF analysis and serum studies. Neurologic exam on admission was notable for severe appendicular ataxia and fatigable end-gaze direction-changing horizontal nystagmus. FDG-PET/CT scan was unremarkable and repeat lumbar puncture revealed 2 WBCs/mm3, 148 RBCs/mm3, glucose 70 mg/dL, protein 37.7 mg/dL and negative flow cytometry/cytopathology. Standard CSF JC virus PCR testing was negative, but ultrasensitive TaqMan real-time JC virus PCR testing was positive, consistent with JC virus-related GCN.
Conclusions: Because of the diagnostic challenges in identifying GCN, a high threshold of suspicion should be maintained in patients with an immune-suppressing condition such as lymphoma or on immune-suppressing agents such as rituximab, even shortly after initiation of therapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


