Leonard Ebah, Prasanna Hanumapura, Deryn Waring, Rachael Challiner, Katharine Hayden, Jill Alexander, Robert Henney, Rachel Royston, Cassian Butterworth, Marc Vincent, Susan Heatley, Ged Terriere, Robert Pearson, Alastair Hutchison
{"title":"A Multifaceted Quality Improvement Programme to Improve Acute Kidney Injury Care and Outcomes in a Large Teaching Hospital.","authors":"Leonard Ebah, Prasanna Hanumapura, Deryn Waring, Rachael Challiner, Katharine Hayden, Jill Alexander, Robert Henney, Rachel Royston, Cassian Butterworth, Marc Vincent, Susan Heatley, Ged Terriere, Robert Pearson, Alastair Hutchison","doi":"10.1136/bmjquality.u219176.w7476","DOIUrl":null,"url":null,"abstract":"<p><p>Acute kidney injury (AKI) is now widely recognised as a serious health care issue, occurring in up to 25% of hospital in-patients, often with worsening of outcomes. There have been several reports of substandard care in AKI. This quality improvement (QI) programme aimed to improve AKI care and outcomes in a large teaching hospital. Areas of documented poor AKI care were identified and specific improvement activities implemented through sequential Plan-Do-Study-Act (PDSA) cycles. An electronic alert system (e-alert) for AKI was developed, a Priority Care Checklist (PCC) was tested with the aid of specialist nurses whilst targeted education activities were carried out and data on care processes and outcomes monitored. The e-alert had a sensitivity of 99% for the detection of new cases of AKI. Key aspects of the PCC saw significant improvements in their attainment: Detection of AKI within 24 hours from 53% to 100%, fluid assessment from 42% to 90%, drug review 48% to 95% and adherence to nine key aspects of care from 40% to 90%. There was a significant reduction in variability of delivered AKI care. AKI incidence reduced from 9% of all hospitalisations at baseline to 6.5% (28% reduction), AKI related length of stay reduced from 22.1 days to 17 days (23% reduction) and time to recovery (AKI days) 15.5 to 9.8 days (36% reduction). AKI related deaths also showed a trend towards reduction, from an average of 38 deaths to 34 (10.5%). The number of cases of hospital acquired AKI were reduced by 28% from 120 to 86 per month. This study demonstrates significant improvements related to a QI programme combining e-alerts, a checklist implemented by a nurse and education in improving key processes of care. This resulted in sustained improvement in key patient outcomes.</p>","PeriodicalId":91218,"journal":{"name":"BMJ quality improvement reports","volume":"6 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2017-05-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1136/bmjquality.u219176.w7476","citationCount":"32","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ quality improvement reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjquality.u219176.w7476","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 32
Abstract
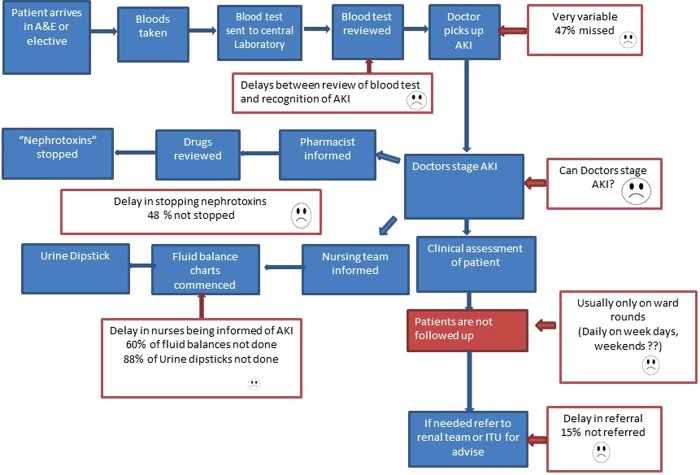
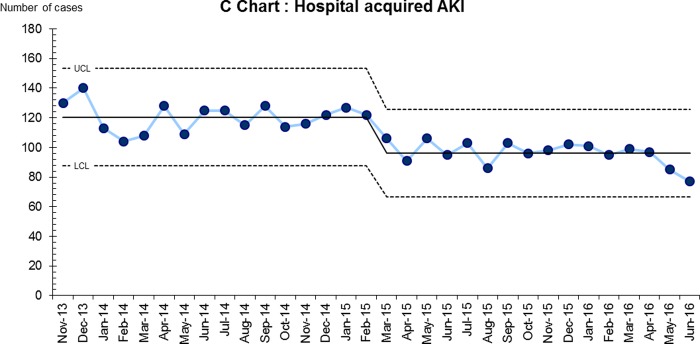
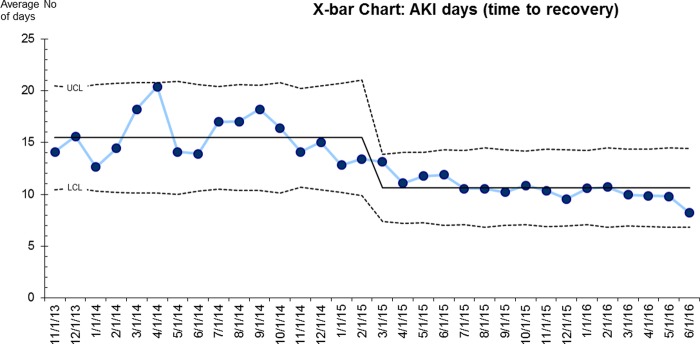
Acute kidney injury (AKI) is now widely recognised as a serious health care issue, occurring in up to 25% of hospital in-patients, often with worsening of outcomes. There have been several reports of substandard care in AKI. This quality improvement (QI) programme aimed to improve AKI care and outcomes in a large teaching hospital. Areas of documented poor AKI care were identified and specific improvement activities implemented through sequential Plan-Do-Study-Act (PDSA) cycles. An electronic alert system (e-alert) for AKI was developed, a Priority Care Checklist (PCC) was tested with the aid of specialist nurses whilst targeted education activities were carried out and data on care processes and outcomes monitored. The e-alert had a sensitivity of 99% for the detection of new cases of AKI. Key aspects of the PCC saw significant improvements in their attainment: Detection of AKI within 24 hours from 53% to 100%, fluid assessment from 42% to 90%, drug review 48% to 95% and adherence to nine key aspects of care from 40% to 90%. There was a significant reduction in variability of delivered AKI care. AKI incidence reduced from 9% of all hospitalisations at baseline to 6.5% (28% reduction), AKI related length of stay reduced from 22.1 days to 17 days (23% reduction) and time to recovery (AKI days) 15.5 to 9.8 days (36% reduction). AKI related deaths also showed a trend towards reduction, from an average of 38 deaths to 34 (10.5%). The number of cases of hospital acquired AKI were reduced by 28% from 120 to 86 per month. This study demonstrates significant improvements related to a QI programme combining e-alerts, a checklist implemented by a nurse and education in improving key processes of care. This resulted in sustained improvement in key patient outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


