Kudakwashe C Takarinda, Charles Sandy, Nyasha Masuka, Patrick Hazangwe, Regis C Choto, Tsitsi Mutasa-Apollo, Brilliant Nkomo, Edwin Sibanda, Owen Mugurungi, Anthony D Harries, Nicholas Siziba
{"title":"Factors Associated with Mortality among Patients on TB Treatment in the Southern Region of Zimbabwe, 2013.","authors":"Kudakwashe C Takarinda, Charles Sandy, Nyasha Masuka, Patrick Hazangwe, Regis C Choto, Tsitsi Mutasa-Apollo, Brilliant Nkomo, Edwin Sibanda, Owen Mugurungi, Anthony D Harries, Nicholas Siziba","doi":"10.1155/2017/6232071","DOIUrl":null,"url":null,"abstract":"<p><p><i>Background</i>. In 2013, the tuberculosis (TB) mortality rate was highest in southern Zimbabwe at 16%. We therefore sought to determine factors associated with mortality among registered TB patients in this region. <i>Methodology</i>. This was a retrospective record review of registered patients receiving anti-TB treatment in 2013. <i>Results</i>. Of 1,971 registered TB patients, 1,653 (84%) were new cases compared with 314 (16%) retreatment cases. There were 1,538 (78%) TB/human immunodeficiency virus (HIV) coinfected patients, of whom 1,399 (91%) were on antiretroviral therapy (ART) with median pre-ART CD4 count of 133 cells/uL (IQR, 46-282). Overall, 428 (22%) TB patients died. Factors associated with increased mortality included being ≥65 years old [adjusted relative risk (ARR) = 2.48 (95% CI 1.35-4.55)], a retreatment TB case [ARR = 1.34 (95% CI, 1.10-1.63)], and being HIV-positive [ARR = 1.87 (95% CI, 1.44-2.42)] whilst ART initiation was protective [ARR = 0.25 (95% CI, 0.22-0.29)]. Cumulative mortality rates were 10%, 14%, and 21% at one, two, and six months, respectively, after starting TB treatment. <i>Conclusion</i>. There was high mortality especially in the first two months of anti-TB treatment, with risk factors being recurrent TB and being HIV-infected, despite a high uptake of ART.</p>","PeriodicalId":30261,"journal":{"name":"Tuberculosis Research and Treatment","volume":"2017 ","pages":"6232071"},"PeriodicalIF":0.0000,"publicationDate":"2017-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5352882/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Tuberculosis Research and Treatment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2017/6232071","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/3/2 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
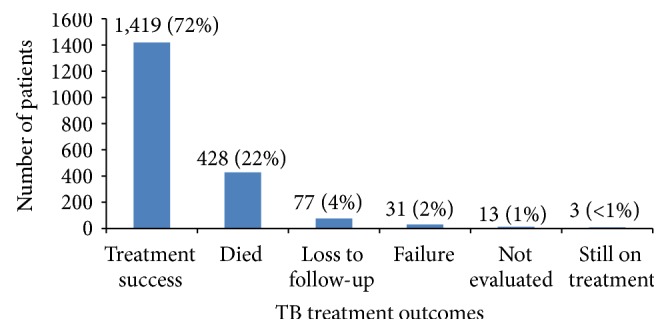
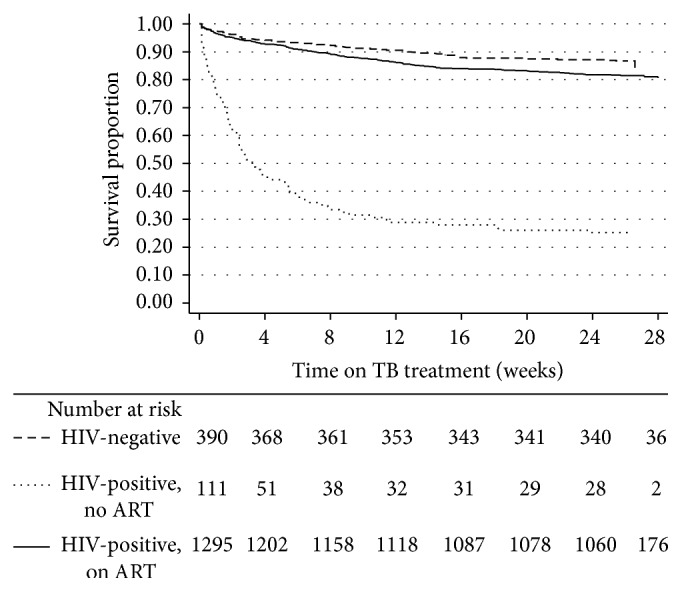
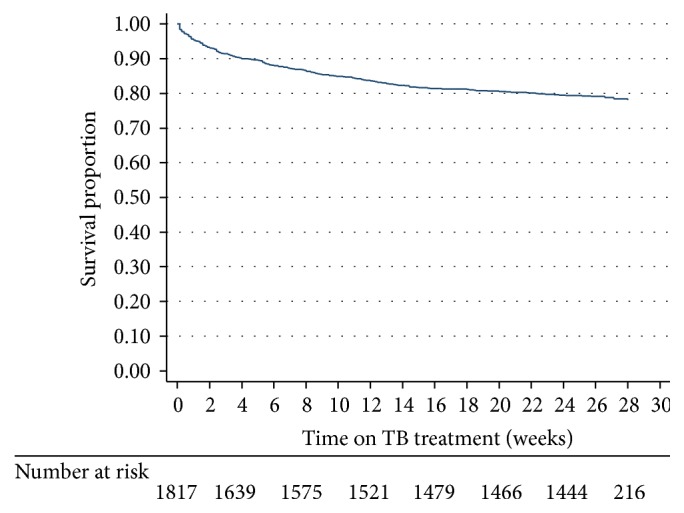
Background. In 2013, the tuberculosis (TB) mortality rate was highest in southern Zimbabwe at 16%. We therefore sought to determine factors associated with mortality among registered TB patients in this region. Methodology. This was a retrospective record review of registered patients receiving anti-TB treatment in 2013. Results. Of 1,971 registered TB patients, 1,653 (84%) were new cases compared with 314 (16%) retreatment cases. There were 1,538 (78%) TB/human immunodeficiency virus (HIV) coinfected patients, of whom 1,399 (91%) were on antiretroviral therapy (ART) with median pre-ART CD4 count of 133 cells/uL (IQR, 46-282). Overall, 428 (22%) TB patients died. Factors associated with increased mortality included being ≥65 years old [adjusted relative risk (ARR) = 2.48 (95% CI 1.35-4.55)], a retreatment TB case [ARR = 1.34 (95% CI, 1.10-1.63)], and being HIV-positive [ARR = 1.87 (95% CI, 1.44-2.42)] whilst ART initiation was protective [ARR = 0.25 (95% CI, 0.22-0.29)]. Cumulative mortality rates were 10%, 14%, and 21% at one, two, and six months, respectively, after starting TB treatment. Conclusion. There was high mortality especially in the first two months of anti-TB treatment, with risk factors being recurrent TB and being HIV-infected, despite a high uptake of ART.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


