{"title":"Hepatectomy Based on Future Liver Remnant Plasma Clearance Rate of Indocyanine Green.","authors":"Yuichiro Uchida, Hiroaki Furuyama, Daiki Yasukawa, Hiroto Nishino, Yasuhisa Ando, Toshiyuki Hata, Takafumi Machimoto, Tsunehiro Yoshimura","doi":"10.1155/2016/7637838","DOIUrl":null,"url":null,"abstract":"<p><p>Background. Hepatectomy, an important treatment modality for liver malignancies, has high perioperative morbidity and mortality rates. Safe, comprehensive criteria for selecting patients for hepatectomy are needed. Since June 2011, we have used a cut-off value of ≧ 0.05 for future liver remnant plasma clearance rate of indocyanine green as a criterion for hepatectomy. The aim of this study was to verify the validity of this criterion. Methods. From June 2011 to December 2015, 212 hepatectomies were performed in Tenri Yorozu Hospital. Of these 212 patients, 107 who underwent preoperative computed tomography imaging volumetry, indocyanine green clearance test, and hepatectomy (excluding partial resection or enucleation) were retrospectively analyzed. Results. There was no postoperative mortality. Posthepatectomy liver failure occurred in 59 patients (55.1%) (International Study Group of Liver Surgery Grade A: 43 cases (40.2%), Grade B: 16 cases (15.0%), and Grade C: no cases). Operative morbidity greater than Clavien-Dindo Grade 3 occurred in 23 patients (21.5%). A low future liver remnant plasma clearance rate of indocyanine green was a good predictor for Grade B cases (area under curve = 0.804; 95% confidence interval, 0.712-0.895). Conclusion. Liver remnant plasma clearance rate of indocyanine green is a valid criterion for hepatectomy. </p>","PeriodicalId":77165,"journal":{"name":"HPB surgery : a world journal of hepatic, pancreatic and biliary surgery","volume":"2016 ","pages":"7637838"},"PeriodicalIF":0.0000,"publicationDate":"2016-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2016/7637838","citationCount":"7","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"HPB surgery : a world journal of hepatic, pancreatic and biliary surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2016/7637838","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/6/23 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 7
Abstract
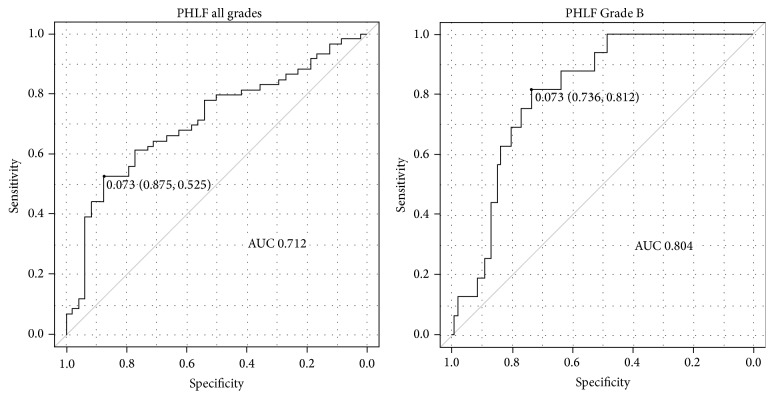
Background. Hepatectomy, an important treatment modality for liver malignancies, has high perioperative morbidity and mortality rates. Safe, comprehensive criteria for selecting patients for hepatectomy are needed. Since June 2011, we have used a cut-off value of ≧ 0.05 for future liver remnant plasma clearance rate of indocyanine green as a criterion for hepatectomy. The aim of this study was to verify the validity of this criterion. Methods. From June 2011 to December 2015, 212 hepatectomies were performed in Tenri Yorozu Hospital. Of these 212 patients, 107 who underwent preoperative computed tomography imaging volumetry, indocyanine green clearance test, and hepatectomy (excluding partial resection or enucleation) were retrospectively analyzed. Results. There was no postoperative mortality. Posthepatectomy liver failure occurred in 59 patients (55.1%) (International Study Group of Liver Surgery Grade A: 43 cases (40.2%), Grade B: 16 cases (15.0%), and Grade C: no cases). Operative morbidity greater than Clavien-Dindo Grade 3 occurred in 23 patients (21.5%). A low future liver remnant plasma clearance rate of indocyanine green was a good predictor for Grade B cases (area under curve = 0.804; 95% confidence interval, 0.712-0.895). Conclusion. Liver remnant plasma clearance rate of indocyanine green is a valid criterion for hepatectomy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


